|
|
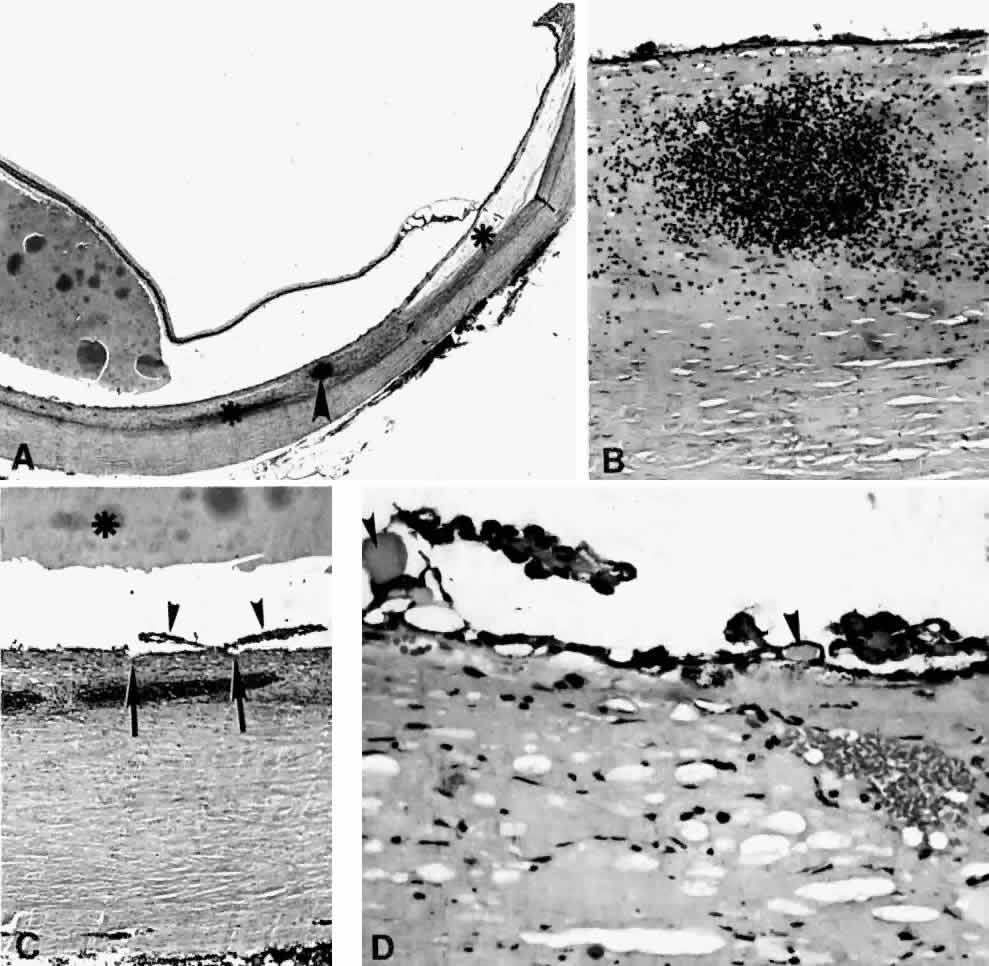
| Fig. 20. A 61-year-old man presented with a 10-day history of decreasing vision in the left eye.96 Examination disclosed a vision of hand motions, an irregularly shallow anterior chamber, closure of the angle, and an intraocular pressure of 45 mmHg. The ora serrata was visible without scleral depression. Ophthalmoscopic examination disclosed two large areas of solid-appearing lesions of the pars plana and anterior choroid (situated superonasally and inferotemporally), detachment of the retina, and a diffuse pigmentary disturbance, which was linear in some areas. Transscleral transillumination disclosed that areas of solid choroidal lesions lit up when viewed through the pupil. Radioactive phosphorus uptake was 16% at 1 hour, 18% at 24 hours, and 44% at 72 hours. The eye was enucleated because of the suspicion of a malignant melanoma. A. An extensive ciliochoroidal effusion (asterisks) showing mild diffuse and marked focal (arrowhead) infiltration of lymphocytes. The equatorial sclera is markedly thickened, and there is a large serous detachment of the retina (H & E, × 17). B. Edematous choroid with a large aggregate of lymphocytes (H & E, × 100). C. The equatorial area shows a thickened sclera, an edematous choroid with diffuse and marked focal aggregates of lymphocytes, localized area of retinal pigment epithelial hypertrophy and hyperplasia (arrowheads), slight folds in the retinal pigment epithelium and inner aspect of the choroid (arrows), and proteinaceous material (asterisk) in the subretinal space (H & E, × 40). D. A choroidal effusion with overlying proliferation of retinal pigment epithelium in nodular and linear configurations. Proteinaceous material is present in some areas in or beneath the retinal pigment epithelium (arrowheads) (H & E, × 180). |