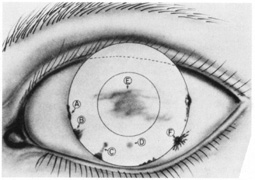
A phlyctenule may occur on the conjunctiva or on the cornea (Fig. 1). The different locations give different symptoms and signs, and they have a different prognosis for vision.
|
| Chapter 8 Phlyctenular Keratoconjunctivitis IRA J. UDELL and JONATHON S. WEYNE Table Of Contents |
|
PREVALENCE PATHOPHYSIOLOGIC CONSIDERATIONS ANIMAL MODELS OTHER CAUSATIVE AGENTS PATHOLOGY CLINICAL MANIFESTATIONS SYMPTOMS SIGNS DIFFERENTIAL DIAGNOSIS TREATMENT PROGNOSIS REFERENCES |
| Phlyctenular keratoconjunctivitis is a nodular affliction characterized
by the formation of a small, circumscribed lesion at the corneal limbus. Duke-Elder
referenced accounts of the condition in Greek, Arabic, French (1722), and English literature (1808).1 At one stage, the lesion may resemble a blister, but the small red nodule
of lymphoid tissue characteristically develops into a microabscess
that ulcerates and heals in 10 to 14 days. Ostler and Lanier2 and Thygeson3 reported the relationship between phlyctenular keratoconjunctivitis and
tuberculoprotein. Thygeson believed that the incidence of phlyctenulosis
on a worldwide basis appeared to parallel the incidence of tuberculosis4: “The occurrence of phlyctenulosis in a child should be considered
a warning of impending clinical tuberculosis.” In a recent prospective
study in Japan, 86 of 112 patients (76.7%) with
phlyctenular disease were associated with tuberculosis.5 Phlyctenular keratoconjunctivitis is now accepted as a morphologic expression of delayed hypersensitivity to diverse antigens. The condition is one of several corneal disorders that arise as an expression of altered immune mechanisms.6 Phlyctenulosis occurs mainly in children and young adults as a result of a hypersensitivity reaction of the conjunctiva or cornea to bacterial products. It can lead to discomfort, extreme photophobia, tearing, and belpharospasm. In severe cases involving the cornea, it may result in ulcers, scarring, vascularization, and even perforation. Disturbance in vision is related to the degree of scarring and to the location of the scarring relative to the visual axis. |
| PREVALENCE |
| Phlyctenular keratoconjunctivitis has been associated in the past with
poor, undernourished, sickly children, with tuberculosis strongly implicated. Duke-Elder
described the pitiable position of these children: “During
the day the child hides away in a dark corner, burying his
face in his hands; and during the night he curls up under the blankets.”1 Phlyctenular keratoconjunctivitis has a worldwide distribution. It is found most commonly during the first and second decades of life in children living in crowded, impoverished quarters. All observers report a higher incidence (60% to 70% of reported cases) in girls than in boys.7,8 Fritz and co-workers9 studied 346 Alaskan native children with corneal scarring apparent in 143 cases. The involvement was bilateral in 112 cases (78%) and unilateral in 31 (22%). Philip and co-workers7 found a characteristic distribution of corneal opacities of varying severity according to age. In their study of 4,635 Eskimos, opacities were infrequent among children younger than 4 to 5 years. However, 53% of school-aged children and 45% of adults exhibited scarring. Opacities were more frequent among females than among males. Of 1197 children who were tested with tuberculin, 93% of those with opacities were reactors to 10 tuberculin units of purified protein derivative (i.e., intermediate-strength tuberculin), whereas only 34% of those without scarring were reactors. Among tuberculin reactors, there was no relation between degree of skin-test hypersensitivity and corneal opacity. Phlyctenular keratoconjunctivitis is uncommon in areas where the incidence of tuberculosis is low. Likewise, the prevalence of corneal opacity was found to be highest in Alaskan households with the greatest crowding and lowest standard of living. As the incidence of tuberculosis in Alaskan natives has fallen from a death rate of 650 in 100,000 population in 1950 to 10 in 100,000 population in 1966, so has the incidence of phlyctenular keratoconjunctivitis, although exact figures are difficult to determine.10 In the United States, where the rate of positive tuberculin test results is relatively low, phlyctenular keratoconjunctivitis may occur in adults as well as in children, and it is likely to occur in patients free of tuberculosis. Sorsby8 reported that phlyctenular keratoconjunctivitis occurs more often in spring and summer than in late autumn or winter. |
| PATHOPHYSIOLOGIC CONSIDERATIONS |
| There is some debate about the pathophysiology and causes of phylctenular
keratoconjunctivitis. A clear analogy exists between phlyctenules of
the conjunctiva and bacterids of the skin.11 Bacterids are nodules in the skin that are comparable histologically, as
well as in their allergic origin, to phlyctenules of the conjunctiva
and cornea. Although the tuberculid is the most common bacterid, dermatologists
describe other types, such as the moniliid and trichophytid, that
result from sensitization to proteins from organisms other than
the tubercle bacillus. The organism is not present in the lid reaction, which
is hypersensitive to organisms present elsewhere in the body. The
tubercle bacillus has not been found in the phlyctenular lesion
itself. Although the precise mechanism by which phlyctenules are produced has not been determined, it is assumed from clinical evidence that the patient has been sensitized to the offending antigen in the past. In patients with tuberculosis, this sensitization presumably occurred as part of a bacteremia from an early infection in the lungs or lymph glands. For nontuberculosis, phlyctenular keratoconjunctivitis caused, for example, by Staphylococcus probably comes from the pathogenic staphylococci that inhabit the lid margins of all people from time to time. The attack of phlyctenular keratoconjunctivitis may be precipitated by the presentation of the antigen to the sensitized ocular tissue, either by the bloodstream in the event of a recrudescence of a focus of infection elsewhere or by an exogenous inoculation of bacteria into the conjunctival sac from the lid margin. |
| ANIMAL MODELS |
| Thygeson and co-workers12 reported that they were not able to reproduce the earlier successes of
Gibson13 and Rosenhauch14 in inducing the formation of phlyctenules by instilling tuberculin or Staphylococcus aureus into the conjunctival sacs of tuberculous rabbits. Consequently, Thygeson
and co-workers concluded that no model was available for studying
the phlyctenules and cellular infiltrates typical of phlyctenular keratoconjunctivitis. Mondino and co-workers,15 however, have reported a successful experimental model of phlyctenulosis in which rabbits were immunized by intradermal and intramuscular injection of phenol inactivated S. aureus. All animals challenged topically with viable S. aureus developed conjunctival hyperemia and edema in the first week. In 26 of the 28 rabbits, vascular invasion of the peripheral cornea from the limbus developed in an average of 33 days (range, 14 to 49 days). In 8 of 22 rabbits, elevated, nodular lesions of the cornea developed in an average of 29 days (range, 14 to 42 days). Elevated, whitish nodular infiltrates developed approximately 3 mm from the limbus in an average of 54 days (range, 43 to 60 days). Nodular infiltrates gradually flattened within a month after topical challenge with S. aureus was discontinued, leaving a vascularized scar. The nodular corneal infiltrates were found in a subepithelial location and were composed of vessels, polymorphonuclear leukocytes, and mononuclear cells, including lymphocytes, plasma cells, and macrophages. The peripheral corneal infiltrates that were separated from the limbus by a lucid interval were found in the anterior stroma beneath the corneal epithelium and were composed of polymorphonuclear leukocytes and mononuclear cells. The pathologic findings seen in the above infiltrates were not suggestive of a direct infection since no gram-positive organisms were found. Further studies in this rabbit model with S. aureus cell-wall immunization were associated with development of corneal phlyctenules and catarrhal infiltrates, suggesting that cell-wall antigen was responsible for these lesions.16 Three major components of S. aureus cell wall are known to exist; however, only rabbits immunized to one of these components, ribitol teichoic acid (RTA), which is coupled to sheep red blood cells, developed corneal phlyctenules after topical application of viable S. aureus.17 Skin tests for delayed hypersensitivity in these RTA immunized rabbits were negative, suggesting that antibody was more important in the development of corneal lesions. Further studies measured serum, tear, and corneal antibody titers to RTA in rabbits immunized by various routes (intradermal subconjunctival, topical) with staphylococcal antigens.18 Analysis of the data suggests that corneal antibody levels to RTA may be influenced by exposure to staphylococcal antigens not only in the external eye but also at sites remote from the eye. |
| OTHER CAUSATIVE AGENTS |
| Infection with parasites has been associated with the development of phlyctenular
keratoconjunctivitis. Al-Hussaini and co-workers19 studied the stools of 471 patients suffering from the phlyctenular disease
and found that 63% of them had Hymenolepis nana ova in their stools, as compared to 11% of the controls. All patients
had H. nana–immune sera. Age incidence and geographic distribution of H. nana infection and phlyctenular keratoconjunctivitis are parallel. Mounting evidence exists for an association of chlamydial infection and phlyctenular disease. Thygeson11 reported a case of lymphogranuloma venereum phlyctenulosis in 1954. Subsequently, Bialasiewicz and Holbach20 described two patients with phlyctenular disease and evidence of chlamydial conjunctival involvement. More recently, Culbertson and co-workers21 studied 17 cases of phlyctenular keratoconjunctivitis in children and teenagers ranging in age from 3 to 18 years. The workup in 10 of these patients included chlamydial cultures and/or monoclonal immunofluorescent antibody stain of conjunctival smears for Chlamydia antigen. Five of these patients (50%) had at least one positive test for Chlamydia. Although nontuberculosis phlyctenular disease is generally presumed to be of staphylococcal etiology, in Culbertson's study random conjunctival and eyelid cultures for bacteria in nine patients were negative; these findings are consistent with our experience. Phlyctenulosis has been associated with pneumococcal and Koch-Weeks conjunctivitis11; however, there have been no such reports in tuberculin-negative subjects. In these last two types of infection, the acute bacterial disease may act as a trigger to precipitate another attack of phlyctenular disease associated with tuberculin allergy. One of the authors has seen bilateral phlyctenular lesions of the limbus and bulbar conjunctiva in an 8-year-old boy 5 days after the onset of varicella with moderate facial and lid involvement. The acute viral process in this case may have been the trigger mechanism of a phlyctenular response to an antigen that the child had been sensitized to in the past. Additional reported microbial agents implicated in phlyctenulosis include Candida albicans, Morax-Axenfeld bacillus, Leishmania, Neisseria gonorrhoeae, and Coccidioides immitis.1,4 Not all bacterial or fungi are known to precipitate phlyctenular keratoconjunctivitis. No case associated with histoplasmosis has been reported. Phlyctenulosis is not produced by the allergens responsible for such forms of allergic conjunctivitis as hay fever conjunctivitis, atopic keratoconjunctivitis, or vernal conjunctivitis. It has not been observed in allergies caused by drugs. |
| PATHOLOGY |
| The pathologic findings of a phlyctenule are lymphocytes, histiocytes, and
plasma cells. In the most acute stages, during which cell death occurs, polymorphonuclear
cells are also found. Follicles, eosinophils, and
giant cells are absent. A number of immunopathologic investigations of phlyctenular disease have been reported. In separate studies, Abu El-Asrar and associates22,23 examined scrapings and biopsy specimens from phlyctenular patients. Scrapings of phlyctenules stained with monoclonal antibodies exhibited T lymphocytes with OKT4/Leu-3a-positive (helper) cells outnumbering OK8-positive (suppressor) cells. On biopsy, the inflammatory cell infiltrate was composed of mononuclear and polymorphonuclear leukocytes suggestive of delayed hypersensitivity. By using immunohistochemical techniques, it was found that lymphocytes (mostly T type) were less abundant than monocyte-derived cells and that there were few B lymphocytes. In Culbertson's study,21 the histology of one bulbar biopsy specimen consisted of a central area of B lymphocytes and histiocytes surrounded by a mantle of lymphocytes, a finding similar to that reported by Hoang-Xuan and associates24 in conjunctival biopsies from patients with ocular rosacea. In rosacea nodules, CD4 helper/inducer cells predominate, a finding believed to be consistent with a type IV hypersensitivity reaction. These findings suggest similarities in the histopathology of phlyctenular and rosacea conjunctival nodule biopsy specimens. |
| CLINICAL MANIFESTATIONS | |
A phlyctenule may occur on the conjunctiva or on the cornea (Fig. 1). The different locations give different symptoms and signs, and they have a different prognosis for vision.
|
| SYMPTOMS |
CONJUNCTIVAL PHLYCTENULOSIS The symptoms of conjunctival phlyctenulosis are mildly to perhaps moderately disturbing. Tearing, irritation, and some itching are mentioned by the patient. If a secondary bacterial infection has occurred, a mucopurulent discharge with sticking of the lids may be described. The symptoms of conjunctival phlyctenulosis last one to two weeks and are often recurrent. The patient with a conjunctival phlyctenule may have had a corneal phlyctenule with the last attack or may have a corneal one on the next attack. CORNEAL PHLYCTENULOSIS The symptoms of phlyctenulosis of the cornea are more severe than those of conjunctival phlyctenulosis. The patient has moderate-to-severe ocular pain, tearing, photophobia, and blepharospasm. The afflicted patient makes every effort to shield the eyes from light. |
| SIGNS | |||||
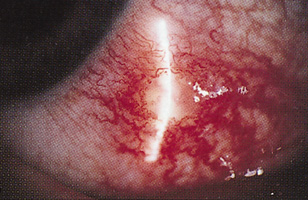
CONJUNCTIVAL PHLYCTENULOSIS The signs of the conjunctival phlyctenule are characteristic. The lesion is found most frequently near the limbus, although it may occur anywhere on the bulbar or, rarely, palpebral conjunctiva (Figs. 2A and 2B). A small, pink-white nodule appears in the center of a hyperemic area. In a few days, the superficial part of the nodule becomes gray and soft. The necrotic center of the lesion sloughs, resulting in a conjunctival defect. The lesion then clears rapidly leaving no scar. Miliary phlyctenular conjunctivitis occurs rarely and is characterized by vast numbers of lesions around the limbus, sometimes becoming confluent.
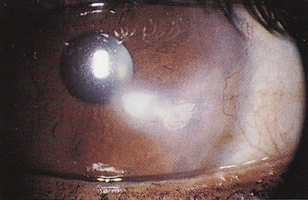
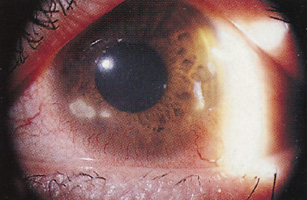
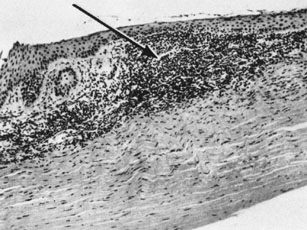
CORNEAL PHLYCTENULOSIS The signs of the corneal phlyctenule are also characteristic (Fig. 3). The lesion usually starts astride the limbus as a white mound bordered on the conjunctival side by a fan of dilated vessels or a marginal ulcer. Clues helpful to the clinician in differentiating these ulcers from catarrhal-type ulcers are the lack of clear intervening cornea between the limbus and ulcer and a perpendicular rather than parallel orientation of the lesion with reference to the limbus. It may remain stationary and evolve through necrosis as a marginal ulcer shelling out (see Fig. 4A) and healing in its original site, or it may travel toward the center of the cornea as a progressing gray, necrotic, superficial fascicular wandering ulcer surrounded by a white infiltrate of the anterior cornea and of tissue over which the ulcer has traveled, resulting in a superficial vascularized scar (see Fig. 4B). Less common manifestations include miliary corneal lesions (minute phlyctenules cover the entire corneal surface), diffuse central infiltrates, and phlyctenular pannus (more prominent inferiorly than superiorly) (Fig. 5). Lymphocytes characterize the corneal phlyctenular infiltrate (Fig. 6). The corneal phlyctenule shells out in 10 to 14 days and leaves a cicatrix according to its severity. The scar may take any form, from an undifferentiated limbal scar to a characteristic, wedge-shaped fascicular scar.
Review of clinical manifestations of phlyctenular keratoconjunctivitis, which are helpful to differentiate it from superficially similar conditions:
|
| DIFFERENTIAL DIAGNOSIS | |
Criteria by which to differentiate phlyctenular keratoconjunctivitis from
various similar disorders are the following:
|
| TREATMENT |
TUBERCULOUS PHLYCTENULOSIS Corneal Phlyctenulosis The treatment of corneal phlyctenulosis is administration of topical corticosteroids. One effective regimen is prednisolone 1%, given every 2 hours during the day for 4 days, followed by administration four times daily for 3 days. Further tapering of corticosteroids is predicated on disease activity. Alternatively, a milder steroid, such as Loteprednol 0.5%, may be used to reduce the risk of steroid-induced elevated intraocular pressure. A cycloplegic agent may be considered for comfort. Dark glasses are helpful. The patient with phlyctenular keratoconjunctivitis should be evaluated for tuberculosis. An intermediate-strength tuberculin test should establish the state of the tubercular reaction. Children and adults younger than 20 years of age with a positive test, as well as any adult with a recently converted test result, should be referred for tuberculosis therapy. If the patient with a positive tuberculin test and phlyctenulosis is a child, a thorough investigation of the family for tuberculosis should be made. Conjunctival Phlyctenulosis A conjunctival phlyctenule that is not causing severe symptoms may be treated by administration of topical astringents. If discomfort is considerable, topical corticosteroids may also be used for this variant of the disease NONTUBERCULOUS PHLYCTENULOSIS If the case seems to be one of nontuberculous phlyctenulosis, the lids should be evaluated for evidence of chronic staphylococcal blepharitis and/or meibomianitis. If one of these is the diagnosis, a vigorous program of lid scrubs with an antibiotic-corticosteroid ointment twice daily for several months, then once daily, should be started. Scales on the lashes or scalp indicate that more must be done, either by the patient or the physician, for the basic problem of staphylococcal-seborrheic blepharitis. Zaidman and Brown25 found oral tetracycline (initial dose, 250 mg two to three times per day until the patient has been asymptomatic for 3 weeks) to be a safe and effective treatment alternative to topical corticosteroids in patients with recurrent episodes of phlyctenular keratoconjunctivitis. Culbertson and co-workers21 further demonstrated the long-term effectiveness of oral tetracycline and erythromycin in the treatment of 17 patients. In this series, 5 of 10 patients investigated for Chlamydia were positive. Importantly, in both studies, oral antibiotic therapy affected long-term remissions of previously chronic disease even after discontinuation of oral tetracycline or erythromycin. This is in contrast to a 50% recurrence of ocular rosacea after discontinuing antibiotics.26,27 Tetracycline treatment is not recommended for children younger than 8 years of age because deposition of tetracycline can discolor the teeth. Other unwanted side effects of oral tetracycline (gastrointestinal upset, cutaneous photosensitivity, and, infrequently, fatty liver degeneration or benign intracranial hypertension) are dose related and resolve once the medication is stopped. Erythromycin may be a reasonable alternative agent, particularly in children. Evidence for the significant presence of hypersensitivity to other agents can be gained by a skin test to Coccidioides (0.05 mL intradermally, read 3 days later), accompanied by a chest roentgenogram, cultures of the lid margins, chlamydial cultures, or immunofluorescent antibody studies and, in appropriate situations, stool examinations for parasites such as Hymenolepis nana. Future treatment may include immunomodulators such as topical cyclosporine. The authors have anecdotal experience suggesting a role for topical cyclosporine ophthalmic emulsion 0.05% for phlytenular keratoconjunctivitis and other ocular surface hypersensitivity diseases. Additional clinical and laboratory study will be necessary to further elucidate the mechanism of action and role T cell suppressors in ocular surface inflammatory disorders. |
| PROGNOSIS |
| Figures on the rates of blindness from phlyctenular keratoconjunctivitis
before the advent of corticosteroids are meaningless for present-day
practice because the use of corticosteroids in the treatment has changed
the prognosis for the disease. The incidence of blindness and visual
impairment since the advent of effective medication has not been established. Most
patients respond favorably to therapy, but, without treatment, phlyctenular
keratoconjunctivitis is a potentially blinding disease. Although
rare, phlyctenular corneal perforation has been reported—by
Ostler28 in one patient and Culbertson and co-workers21 in three patients. Corneal scarring can be successfully managed with penetrating
keratoplasty. As reported by Smith and co-workers,29 clear grafts were obtained in 14 of 18 patients (79%) in
their series. Much remains to be learned about phlyctenular keratoconjunctivitis, including (1) the explanation for the focal nature of the disease; (2) the mechanisms by which attacks are precipitated; (3) the particular proclivity of the tuberculoprotein to produce phlyctenules, despite the ability of many bacterial proteins to sensitize ocular structures; (4) the mechanisms of producing phlyctenules; (5) the reasons and ways limbal phlyctenules migrate into the cornea; (6) the absence of uveal tract inflammation; (7) the spontaneous desensitization that seems to occur in adults; and (8) the absence of phlyctenulosis in animals, despite the fact that tuberculosis and other granulomatous diseases that produce significant allergies or infection are common in animals. The advent of a satisfactory animal model like that of Mondino and co-workers will hopefully provide answers to some of these important questions. |