| Bacterial infections of the lid margins, especially staphylococcal infections, are
common. STAPHYLOCOCCAL LID INFECTIONS Staphylococcal blepharitis is not self-limited and is difficult to eradicate
successfully.4 It is a common cause of chronic conjunctivitis, recurrent epithelial keratitis, and
recurrent morbidity. The patient is frequently beset with
symptoms of photophobia, pain, tearing, redness, blurred vision, and
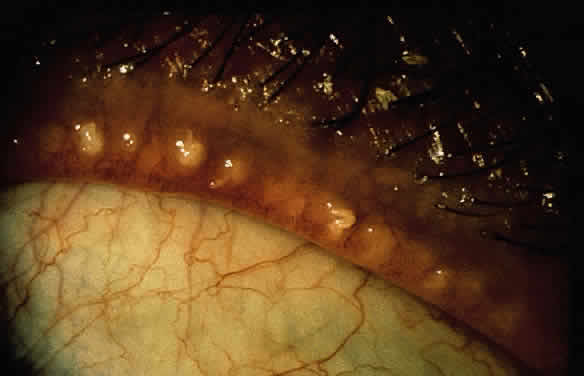
discharge. The infection is characterized by one or more of the following features2: - Ulcerations at the base of the eyelashes: The ulceration is preceded by a folliculitis of the pilosebaceous unit. Fibrin, which
exudes from the base of the ulcer, usually masks the presence
of the ulcer.
- Collarettes: Collarettes are small, thin, fibrinous scales that surround the eyelash
like a small piece of paper impaled on a stick. The collarette is formed
by the fibrin that covers the base of the ulcer. It usually surrounds
the eyelash and may be carried away from the surface of the skin
as the lash grows (Fig. 5).
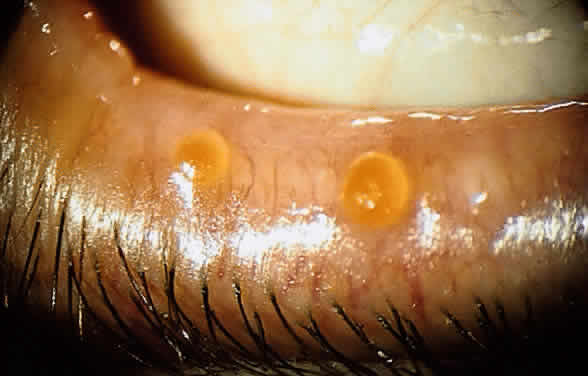
- Localized poliosis or canities (whitening) of individual eyelashes: Poliosis occurs from staphylococcal damage to the pilosebaceous unit (Fig. 6).
- Short, misdirected, broken, sparse, or missing eyelashes: The hair follicles are often damaged by the staphylococcal infection. Lashes
produced in damaged hair follicles are often short, misdirected, and
broken. Large areas where eyelashes are absent are commonly found.
- External hordeolum (style): An external hordeolum represents an abscess of a gland of Zeis. Pain, redness, and
swelling occur. The pain is proportional to the degree of
swelling. The abscess points to the skin at the lid margin.
- Internal hordeolum: An internal hordeolum is often caused by a staphylococcal infection. The
infection occurs within the meibomian gland and often produces intense
pain and swelling. The lesion may eventually drain through the skin
or conjunctiva.
- Multiple, recurrent chalazia: Multiple or recurrent chalazia are often caused by staphylococcal infections
of the meibomian glands. The staphylococcal infections cause inflammation
and edema of the neck of the gland, with resulting inspissation
of the meibomian gland and, eventually, chalazion formation.
- Fine, epithelial keratitis: A fine, epithelial keratitis of the lower half of the cornea is commonly
associated with staphylococcal blepharitis. The keratitis is more severe
in the morning and often clears during the daytime.
- Catarrhal corneal infiltrates or ulcers: Catarrhal corneal infiltrates usually occur at the 2-, 4-, 8-, and 10-o'clock
areas of the peripheral cornea. They are usually separated from
the limbus by a lucid interval and commonly progress to ulceration of
the overlying epithelium. These lesions are sterile and represent immunologic
responses to bacterial antigens. The clinical diagnosis of staphylococcal
blepharitis is verified by culture, which reveals many S. aureus organisms on the lid margins. The bacterial cultures and antibiotic sensitivity
patterns also are useful in suggesting the appropriate antibiotic
for treatment.
 Fig. 5. Anterior lamella lid disease due to staphylococcal infection. Note collarette
in the center of the photograph. Fig. 5. Anterior lamella lid disease due to staphylococcal infection. Note collarette
in the center of the photograph.
|
 Fig. 6. Anterior lamella lid disease with acute folliculitis, lash misdirection, lash
loss, erythema, and tylosis. Fig. 6. Anterior lamella lid disease with acute folliculitis, lash misdirection, lash
loss, erythema, and tylosis.
|
To treat staphylococcal blepharitis, do the following: - Direct the patient to remove all fibrinous crusts and discharge from the
lid margin with lid scrubs, as described under seborrheic blepharitis.
- Have the patient then apply a suitable antibiotic ophthalmic ointment to
the base of the eyelashes at nighttime.
- Continue treatment for 6 weeks, and then reculture the lid margin and change
antibiotics as necessary according to the results of the antibiotic
sensitivity pattern.
In some instances, systemic antibiotics are necessary to control symptoms. Fusidic
acid ointment has been shown to be an effective treatment
for various staphylococcal species, but this ointment is not available
in this country. The skin of the eyelid may be involved by impetigo contagiosa, infectious
eczematoid dermatitis, or staphylococcal scalded skin syndrome. Impetigo Contagiosa Impetigo contagiosa of the skin of the eyelid is usually associated with
infection of the face. The infection begins as a small macule that enlarges, vesiculates, and
then pustulates. Bullae can form and become
crusted. The crusts are usually thin and varnish-like, which helps to
differentiate the infection from streptococcal impetigo, in which the
crusts are thick and honey-colored. The infection is more common in children
younger than 6 years of age. Local treatment of staphylococcal impetigo is usually sufficient. If the
diagnosis of staphylococcal impetigo is in doubt, however, treat the
patient with systemic antibiotics, since streptococcal skin infections
can lead to glomerulonephritis. For local treatment, do the following: - Cleanse the affected area with mild soap and water followed by warm soaks
to help loosen the crusts.
- Have the patient apply erythromycin or bacitracin ophthalmic ointment to
the involved area two to four times daily.
- If a favorable response is not obtained after 3 to 4 days, change the antibiotic. Systemic
antibiotics are sometimes necessary.
Infectious Eczematoid Dermatitis An infectious eczematoid dermatitis is similar to, and often confused with, contact
dermatitis. Vesiculation, pustulization, crusting, and lichenification
are characteristic. The skin of the entire eyelid may be
involved. Conjunctivitis and keratitis can also occur. The patient is
sensitized to the staphylococcal products, which serve as haptens. Topical antibiotic ophthalmic ointment may suffice, although systemic antibiotics
such as erythromycin or dicloxacillin (0.250 g) four times
daily might be necessary. Topical corticosteroids are deemed by some practitioners
to help control the skin eruption. Staphylococcal Scalded Skin Syndrome Staphylococcal scalded skin syndrome (Ritter's disease) occurs in
young children. The entire body, beginning with the face and the flexural
creases of the neck, axilla, and groin, is involved. The eruption
is preceded by a short prodromal period of malaise, fever, irritability, and
skin tenderness. A diffuse scarlatiniform erythema develops quickly, followed
by separation of the epidermis. A positive Nikolsky's
sign is characteristically present. To treat staphylococcal scalded skin syndrome, do the following: - Give oral dicloxacillin (50 to 100 mg/kg/day) in four divided doses or
erythromycin base (40 mg/kg/day) in four divided doses.
- Keep the denuded areas moist with sterile Burow's solution or normal
saline solution.
MIXED BLEPHARITIS Mixed blepharitis is caused by seborrhea with superimposed staphylococcal
infection. It is a common condition, and it is probably the most common
form of blepharitis. The symptoms and signs of seborrhea and staphylococcal
infection are both present. Both conditions are treated as
outlined earlier. ANGULAR BLEPHARITIS (DIPLOBACILLARY BLEPHARITIS, STAPHYLOCOCCAL BLEPHARITIS) Angular blepharitis is usually associated with angular conjunctivitis of
the medial or lateral conjunctiva. Fissuring, scaling, lichenification, and
redness are evident at the external or internal canthus. There
is usually also a mild mucoid discharge. In warm climates, the diplobacillus of Morax-Axenfeld (Moraxella [Moraxella] lacunata), a large, gram-negative, square-ended bacillus that usually occurs in
pairs, is implicated as causing the infection. In colder climates, however, S. aureus is commonly implicated. Treat the angular blepharitis as outlined earlier under staphylococcal
infections. β-HEMOLYTIC STREPTOCOCCAL LID INFECTIONS Impetigo contagiosa, caused by β-hemolytic streptococcus, may spread from the face to
the eyelids. The infection is superficial and similar in many respects
to staphylococcal impetigo, except that in the former the bullae tend
to rupture more readily, the crusts are thicker and honey-colored, and
there is usually a more pronounced regional lymphadenopathy. However, the
two forms can be accurately differentiated only by cultures. Acute
glomerulonephritis can be associated with streptococcal impetigo, mandating
that the infection be treated with systemic antibiotics (e.g., oral dicloxacillin; erythromycin stearate or free base [0.250 g] four
times daily).1 Erysipelas is a comparatively deep skin infection caused by Streptococcus pyogenes. It is characterized by warm, red, swollen lesions with sharply raised, readily
outlined borders. Vesicles or bullae are often present. Associated
systemic symptoms and signs are headache, joint pains, chills, and
fever. Treat erysipelas with systemic antibiotics, as outlined under
impetigo contagiosa. Infectious eczematoid dermatitis may be caused by streptococcal infections. It is similar to infectious
eczematoid dermatitis caused by staphylococcal infections, and should
be managed in a similar fashion. PSEUDOMONAS SPECIES, PROTEUS SPECIES, AND COLIFORM ORGANISMS The lid margin of the immunocompromised host occasionally is infected with
gram-negative rods, such as Pseudomonas sp., Proteus sp., or coliform organisms. The diagnosis is made by culture, since the
infection produces no identifying features. In many instances these
organisms can be cultured from healthy-appearing lid margins.5 Have the patient use lid scrubs, as outlined earlier, followed by the application
of gentamicin or other suitable antibiotic ophthalmic ointments, depending
on the findings of the antibiotic sensitivity pattern. In neonates and severely immunocompromised patients, ecthyma gangrenosum, a circumscribed, ulcerated, hemorrhagic lesion caused by Pseudomonas sp., can occur on the eyelid.5 The lesions can cause extensive sloughing of the eyelid. Patients with
ecthyma gangrenosum must have their immunosuppression reversed, when
possible, and should be treated with intravenous (IV) antibiotics, such
as gentamicin (3 to 7 mg/kg/day IV) or ticarcillin (200 to 300 mg/kg/day
IV). |