
|
|
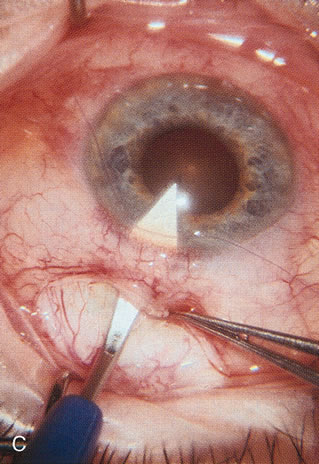
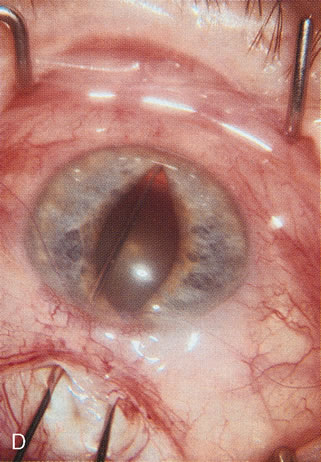
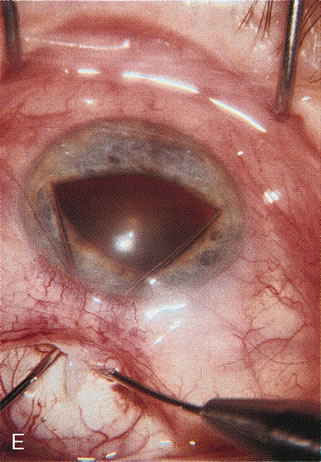
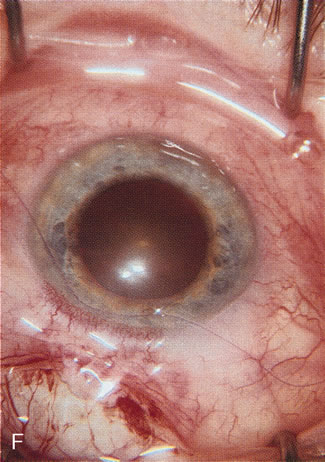
| Fig. 14. Management of intraoperative miosis.One of the most common explanations for a surgical complication related to lens extraction is insufficient pupillary dilatation and the failure to adequately deal with it (Table 4). A. Multiple minisphincterotomies are made with capsulotomy or iris scissors, with only part of the sphincter being incised. However this requires a fairly large scleral opening and controlling the extent of the radial iridotomy is difficult. These maneuvers are difficult in a narrow-angled eye. B. Self-retaining iris clips require four paracentesis tracts and additional time to insert. Pupil function postoperatively is usually excellent. The hooks can be easily placed through a paracentesis track made with a super sharp. The track should start at the edge of the limbus and be directed toward the center of the pupil so as to avoid the hooks being too anterior resulting in upward tenting of the iris when retracted. If the track is too oblique, aiming at the root of the iris, it is impossible to engage the hook onto the edge of the pupil. The surgeon must carefully retract these hooks when finished or occasionally the hook will tear the anterior capsule. C. Appearance of pupil before stretching technique. D. A two-instrument pupil stretching technique is efficient, simple and allows adequate visualization for most patients. Occasionally, a pupillary membrane must be lifted off the capsule with a viscoelastic and then removed before engaging the pupillary border. Use two Kuglen hooks, one with a straight handle, the other angled. Insert the straight hook first and engage the iris at 12 o'clock and engage the iris at 6 o'clock with the angled hook. A slow steady push toward the respective limbus will stretch the pupil. The pupil is stretched approximately 80% of the translimbal distance. E. If the pupil is not large enough after the first stretch, cross the instruments at the wound margin and engage the pupil border in the iris plane at 3 and 9 o'clock; repeat the same motion. This creates multiple tiny sphincterotomies leaving a functional 3.5-mm pupil. If the pupil is extremely miotic, fibrotic and bound down, only stretch the pupil 60% of the translimbal distance, otherwise an atonic pupil is more likely to occur. F. The pupil is now adequately dilated by mechanical means to safely proceed with surgery. |