|
|
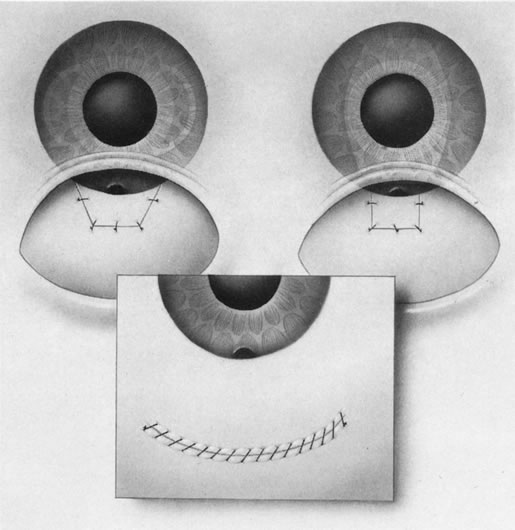
| Fig. 19. Trapezoidal flap and insertion of rigid PMMA IOL in place of a foldable IOL. If the surgeon elects to insert a rigid IOL instead of a foldable one, a different course of action is required. Construct the scleral flap in a trapezoidal fashion to allow for a larger wound for IOL insertion. Mark 5.5 mm at the limbus with a caliper and use a razor blade to connect the posterior lateral edge of the scratch incision to the limbal mark on both sides. Dissect the flap with a razor blade to the limbus and extend the wound with a 5.1-mm keratome. Insert a 6 mm one-piece polymethylmethacrylate (PMMA) IOL into the capsular bag and rotated as needed. Instill a short-acting miotic into the anterior chamber. The assistant retracts the scleral flap exposing the scleral bed. Grasp the anterior edge of the bed with a 0.12-mm forceps, and with the other hand incise with a super-sharp blade the tissues 1 mm from the anterior lip, parallel to the lip of the wound. Insert a Kelly punch into this slit and remove a block of trabecular tissue, followed by a peripheral iridectomy. This leaves a corneal bridge that prevents long-term sliding of the wound. Close the scleral flap, remove viscoelastic, and tie the preplaced sutures while estimating flow. In this example of a limbus-based conjunctival flap, the globe is rotated inferiorly with the corneal traction suture, and the wound is closed in two layers with absorbable sutures on a vascular needle. The double-layer closure prevents wound leaks that are more likely to occur with antimetabolite usage. Insufflate the chamber with balanced salt solution through the paracentesis track and check the bleb for leaks. Remove the traction suture, inject subconjunctival antibiotic and corticosteroid and patch and shield the eye. |