|
| Chapter 65 Degeneration and Atrophy of the Iris DEEPAK P. EDWARD Table Of Contents |
|
PATHOLOGY OF IRIS ATROPHY CAUSES AND CLINICAL FEATURES AGE-RELATED CHANGES CLINICAL FEATURES TREATMENT PRIMARY IRIS ATROPHIES SECONDARY IRIS ATROPHIES OTHER SECONDARY ATROPHIES REFERENCES |
| PATHOLOGY OF IRIS ATROPHY | |
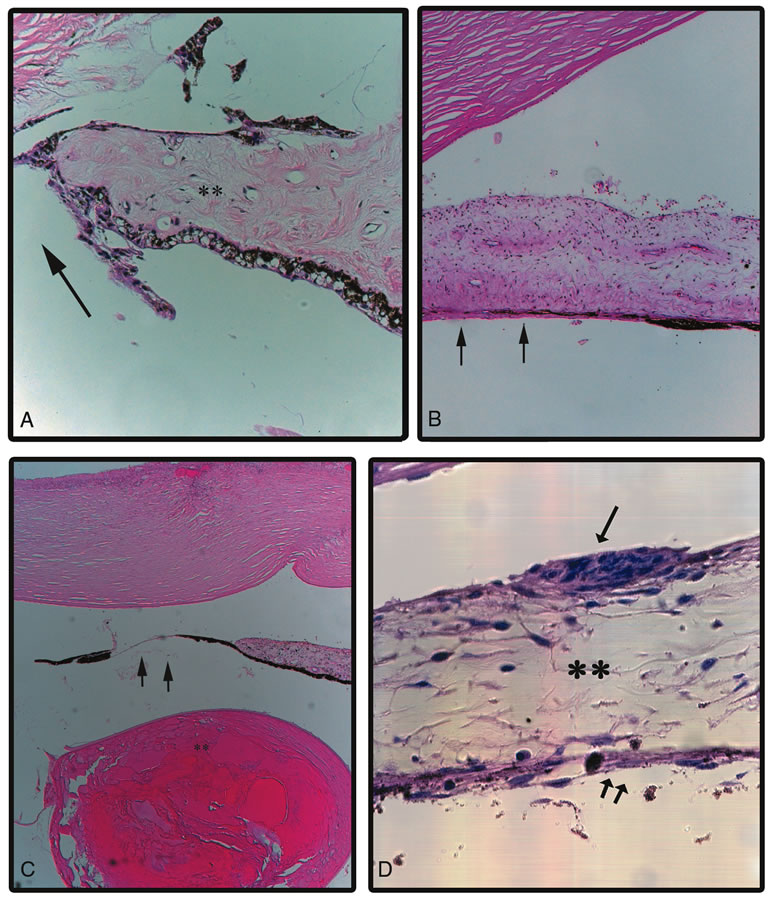
Pathologic changes in the iris and consequent clinical appearance may vary
depending on the layer of the iris involved. Iris stromal atrophy
causes stromal thinning and results in loss of iris crypts and the surface
texture. Also accompanying degeneration or loss of stromal melanocytes
might alter the color of the iris. Degenerative changes may include
loss of normal iris stroma being replaced collagenous tissue that
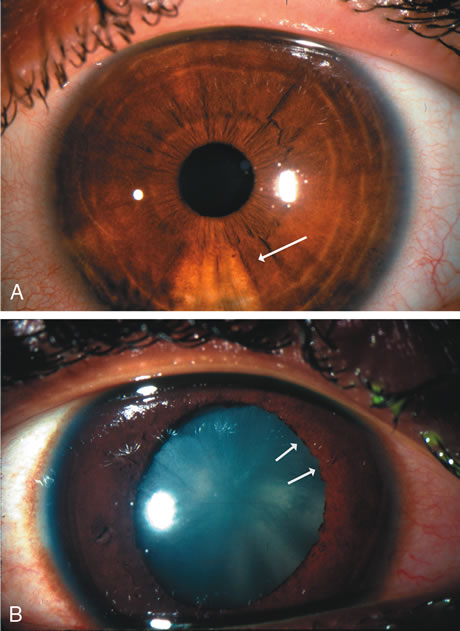
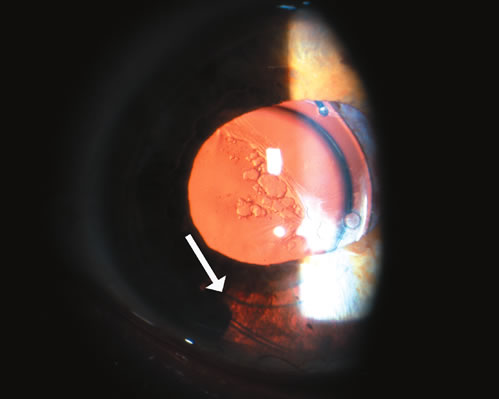
might appear whitish in color on slit lamp examination (Fig. 1A). Iris atrophy may be limited to the iris pigment epithelial layer (Fig. 1B). This may be seen in conditions such as pigmentary glaucoma,1 diabetic changes2 in the iris as well as chafing of the posterior iris surface after sulcus
implantation of an intraocular lens3,4 (Fig. 1C). Such localized atrophy of the iris pigment epithelium would clinically
show normal or slightly altered anterior iris and the presence
of transillumination defects in the iris. Iris atrophy might also involve
both stroma and the iris pigment epithelium where there might be
focal or generalized loss of both layers giving a moth-eaten appearance
to the iris or polycoria such as is seen in iridocorneal endothelial
syndrome5 (Fig. 1D).
|
| CAUSES AND CLINICAL FEATURES |
| Table 1 lists the specific forms and causes of iris atrophy. Specific forms of
iris atrophy and their clinical presentations are described below.
Table 1. Causes of Iris Atrophy and Degeneration Congenital, familial, genetic,age-related
|
| AGE-RELATED CHANGES |
| Atrophy of both the iris stroma and the pigment epithelial layer occurs as a natural aging process. Elderly patients may note a change in the iris to a more blue color but these changes are usually not symptomatic. |
| CLINICAL FEATURES | |
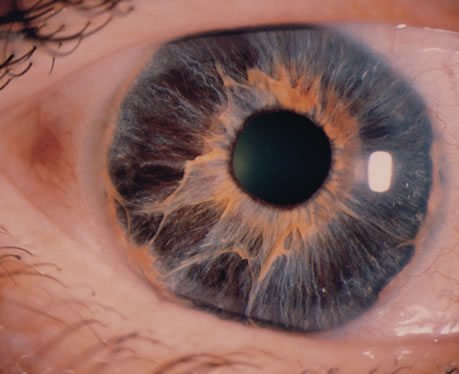
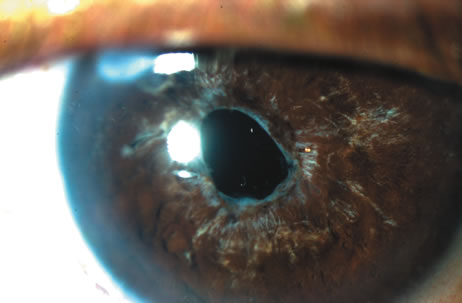
On slit-lamp biomicroscopy, a generalized thinning of the iris stroma, flattening
of the architecture and a disappearance of the crypts, especially
in the pupillary zone is noted (Fig. 2). The brown sphincter muscle becomes visible, and the entire pigment
epithelial layer is easily seen. The pigment epithelial layer itself
may show diffuse depigmentation and, occasionally, focal areas of proliferation. The
pupillary ruff often develops a moth-eaten appearance; granules
of pigment may be seen scattered over the anterior
iris surface, the anterior lens capsule, the endothelial surface of the
cornea, and the trabecular meshwork. The red fundus reflex may be seen
through the patchy areas of iris atrophy.
Functional changes are not clinically significant, although the so-called senile miosis and relative immobility of the pupil are common findings. The causes of these findings are probably related to hyalinization of the stroma and preferential atrophy of the dilator muscle, which arises from the iris pigment epithelium. These senile changes are believed to occur more frequently and earlier in eyes with pseudoexfoliation of the lens capsule. |
| TREATMENT |
| Complications do not result from these changes, and no therapy is warranted except for reassuring the patient that the change in iris color does not represent any disease process. |
| PRIMARY IRIS ATROPHIES | ||
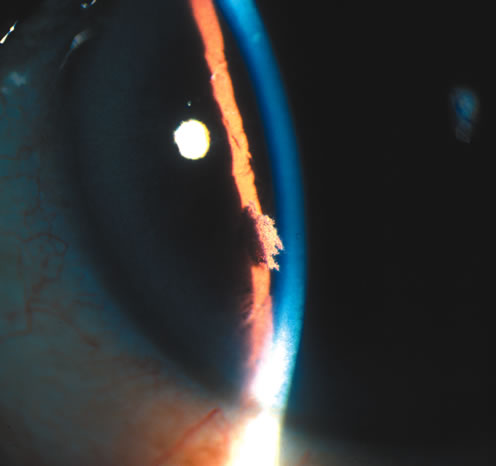
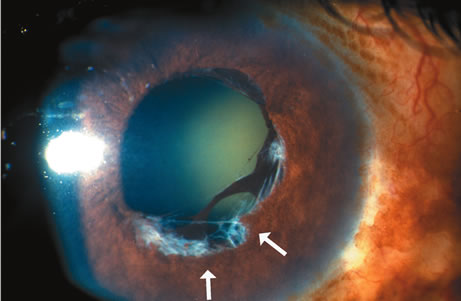
IRIDOSCHISIS Clinical Features Iridoschisis is a rare condition that involves the iris stroma. The term iridoschisis is used when there is a split causing a cleft to occur in the iris stroma. The iris pigment epithelium and dilator muscle posteriorly are unremarkable. Histopathology including transmission electron microscopy shows marked atrophy of the iris stroma with separation of its anterior and posterior layer. The iris vasculature appears unremarkable.6,7 Iridoschisis mainly occurs in elderly8–10 but isolated cases have been reported in young patients after concussive injury.11 It has also been reported to occur as a familial condition,12 has been associated with microphthalmos,13,14 interstitial keratitis,14,15 use of miotics,8 keratoconus,16 and lens subluxation.17 Slit-lamp examination reveals iris stromal fibers and blood vessels that remain attached to one portion of the iris with the loose ends floating freely in the anterior chamber, producing the so-called shredded-wheat appearance. The location of iridoschisis is often inferior (Fig. 3).
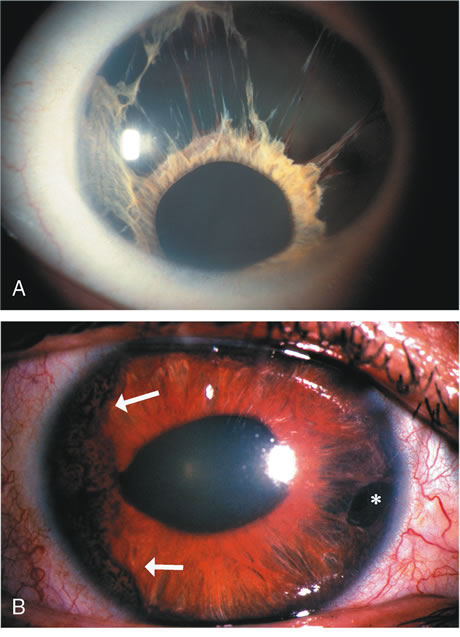
Iridoschisis may be associated with glaucoma in approximately 50% of the patients.8,18 The role of glaucoma in the pathogenesis of iridoschisis is, however, controversial. It has been hypothesized that iridoschisis may result in a secondary form of glaucoma where the ruptured stromal fibers form anterior synechiae that block trabecular outflow.19 Others believe that the schisis in the iris is a result of iris stromal ischemia following acute elevation of intraocular pressure. Ultrasound biomicroscopy demonstrates narrowing of the angle, diffuse or discrete iris stromal changes with intact pigment epithelium in familial iridoschisis and it is suggested that such patients may be predisposed to angle closure glaucoma.20 Treatment Except for being alert to the possible relationship to angle-closure glaucoma, no specific therapy is warranted for iridoschisis. IRIDOCORNEAL ENDOTHELIAL SYNDROME Etiology Iridocorneal endothelial syndrome (ICE) denotes a spectrum of ocular disorders that includes progressive essential iris atrophy, Chandler's syndrome, and iris-nevus syndrome of Cogan-Reese.5,21–26 It is included in this chapter because these ocular disorders were previously referred to as the essential iris atrophies. The defect appears to be an abnormality of the corneal endothelium, that results in endothelial cell proliferation causing a monolayer of endothelial cells with an underlying basement membrane to extend across the anterior chamber angle and onto the anterior surface of the iris.27–29 The contracture of the membrane results in iris atrophy and defects as well as the peripheral anterior synechiae that causes secondary glaucoma. An inflammatory and/or viral process has been implicated in the pathogenesis of the syndrome. Alvarado et al.30 used the polymerase chain reaction to detect herpes simplex virus DNA in corneal specimens with the ICE syndrome and the herpes simplex virus (HSV) was also isolated from the aqueous humor of a patient with ICE syndrome.31 Endothelial cell metaplasia is demonstrated in corneal specimens with ICE syndrome as shown by expression of various cytokeratins that are expressed in the corneal endothelium.32,33 Clinical Features It is the appearance of the iris that divides this spectrum of diseases into clinical variations.34 The most familiar form is progressive iris atrophy or essential iris atrophy in which there is marked corectopia, extensive and progressive atrophy of the iris producing a pseudopolycoria (Fig. 4A).22,27,28 In Chandler's syndrome, the iris shows only mild stromal atrophy and/or corectopia with predominant corneal changes.25 In the iris-nevus syndrome of Cogan-Reese, nodular or diffuse pigmented lesions are present on the surface of the iris in association with varying degrees of corectopia and atrophy of the iris (Fig. 4B).24,26 In the iris-nevus syndrome, these benign lesions of the iris may be confused with malignant melanoma.
Although there is some overlapping of findings in this group of disorders, the complaint of the patient depends on which variant dominates. For example, in progressive iris atrophy, the complaint is the change in the appearance of the iris (i.e., polycoria); in Chandler's syndrome, the patient complains of visual disturbance secondary to the corneal edema; in iris-nevus syndrome, the acquired heterochromia is the usual complaint. Examination of these patients reveals the aforementioned iris changes, and common to all variants is the peripheral anterior synechiae and secondary glaucoma. On slit-lamp biomicroscopy there is a fine, stippled appearance of the posterior cornea resembling fine-hammered silver, similar to but less coarse than that of Fuchs' dystrophy. Clinical specular microscopy often reveals the abnormality of the corneal endothelial cells, characterized by variable degrees of pleomorphism in size and shape.29–35 Unilateral desquamating endotheliopathy may represent an incipient form or a form fruste of the iridocorneal endothelial syndrome.36 Treatment Management is directed to control of the corneal edema and the secondary glaucoma. The corneal edema if present is first treated by medical means (hypertonic saline) and may in due course may need penetrating keratoplasty. Management of the secondary glaucoma is challenging and is first treated with topical medications to control the elevated intraocular pressure. Such patients might eventually need filtration surgery or a seton procedure. Multiple procedures are often needed to achieve successful control intraocular pressure.37,38 |
| SECONDARY IRIS ATROPHIES | ||||||
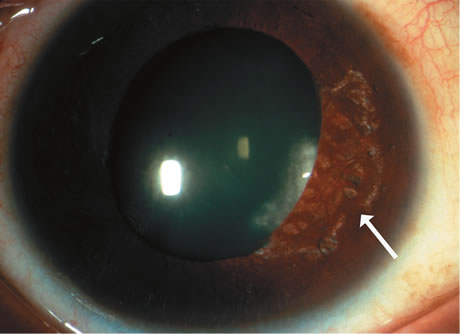
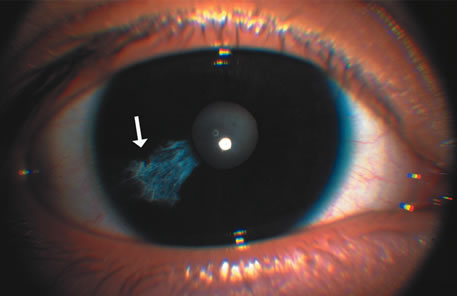
INFLAMMATORY AND TRAUMATIC A diffuse atrophy often follows inflammatory diseases of the iris, including Fuchs' heterochromic uveitis,39,40 nonspecific iritis (Fig. 5), herpes zoster,41,42 and herpes simplex.43 The iris becomes gray and dull, as in senile atrophy, but the pigment epithelium is usually more resistant to these changes. In fact, ectropion uveae is a common finding. Aggregations of pigment are often seen scattered on the various tissues of the anterior segment, and sclerosed white lines often replace the vessels.
Segmental iris atrophy might also occur from anterior segment inflammation45 This has been most commonly described with herpes zoster virus41,42 (Fig. 6A) and also been seen after herpes simplex,43 bee stings,44 and cytomegalovirus infections.45 The atrophy at times is limited to a focal segment and holes may result. Focal iris atrophy may also be seen in granulomatous disease such as tuberculosis and syphilis. A wide variety of atrophic iris changes may be seen in leprosy.46 The findings that best distinguish these postinflammatory secondary atrophies from mere senile atrophy are the presence of anterior and posterior synechiae.
The iris atrophy that follows trauma resembles that which occurs after inflammation, although distortion of the pupil is more common as a results of sphincter tears (Figure 6B). SURGICAL One of the more common reasons for focal iris atrophy in recent years is found in eyes that have undergone extracapsular cataract extraction with placement of an intraocular lens implant.45,47 This is an erosion phenomenon that occurs with anterior chamber lens and sulcus fixated lens (Fig. 7).48,49 Iris atrophy is also seen commonly around surgical or laser iridectomies.
More recently inadvertent iris burns resulting in iris atrophy have been seen after laser treatment to the posterior pole (Fig. 8) and focal atrophy after thermotherapy for retinoblastomas.50
GLAUCOMATOUS Segmental iris atrophy associated with slight dilatation and irregularity of the pupil is characteristic after an acute attack of angle-closure glaucoma.51 The segmental nature is secondary to necrosis of the sphincter muscle (Fig. 9). A splitting of the stroma may occur (iridoschisis), and/or hole formation may ensue.
Iris atrophy may also be associated with pigmentary glaucoma and pigment dispersion syndrome where peripheral radial transillumination defects representing iris pigment epithelial atrophy are noted.52 In addition exfoliation syndrome may be associated with atrophic changes of the iris at the pupillary border with associated transillumination defects.53,54 NEUROGENIC In neurogenic atrophy, such as in association with neurosyphilis or lesions of the ciliary ganglion, the atrophy may start as an alteration in the pigmentation, either depigmentation or focal areas of hyperpigmentation. Thereafter, patchy or generalized atrophy of the stroma develops. In patchy atrophy the pupil is irregular and the part of the pupil corresponding to the atrophic zone has the greatest radius of curvature.55 ISCHEMIC Ischemic atrophy is best characterized by the discrete focal white patches of stromal atrophy occurring at the pupil or between the pupillary margin and the collarette.40–42 It may be associated with sickle cell disease (Fig. 10) and other causes of anterior segment ischemia.56–58 Hypoperfusion can produce a patchy stromal atrophy with secondary micro-neovascularization,59 and an acute primary ischemic iris atrophy can occur with occlusion of the greater vascular circle of the iris.60 An ischemic form of atrophy has also been described with quinine toxicity.61
COMPLICATIONS In all the secondary atrophies, the important clinical complication to keep in mind is the development of synechiae and the potential consequent problems such as pupillary block glaucoma after extensive posterior synechiae or chronic secondary glaucoma as a result of extensive peripheral anterior synechiae. |
| OTHER SECONDARY ATROPHIES |
| Iris atrophy has also been reported to accompany a number of congenital diseases (Table 1) such as arteriohepatic dysplasia (Alagille's syndrome)63 and oculocerebral hypopigmentation syndrome (Cross syndrome).64 |