|
| Chapter 23 Ocular Motility HERSCHEL P. GOLDSTEIN and ALAN B. SCOTT Table Of Contents |
| THE ORBIT | |
The medial orbital walls are generally parallel; the lateral orbital walls
diverge one from the other at an angle of approximately 90 degrees (Fig. 1). The orbits reach adult proportions at age 13 to 15 years, with the visual
axes of the two eyes separated by 60 to 70 mm. The orbits are closer
to one another in infancy, and in some children an especially narrow
interocular distance leads to an appearance of the eyes being crossed, or
esotropia. Growth of the nasal sinuses widens this distance. Displacement
or rotation of the orbits can carry the extraocular muscles
and vary the normal geometry of their action. For example, if the orbits
are rotated in craniofacial disorders, the normal horizontal action
of the horizontal rectus muscles takes on also a vertical action. Imaging
of the bones and muscles by computed tomography (CT) or by magnetic
resonance imaging (MRI) is useful to tell these variations from normal.
|
| BASIC GEOMETRY OF EYE POSITIONS | ||||
NOMENCLATURE Monocular eye movements are called ductions. Binocular eye movements in the same direction are called versions or gaze movements. Normal eyes maintain the same relative alignment in various positions of gaze: comitance. When the eyes move unequally because of muscle weakness or restrictions, incomitance results. Eye movements in contrary directions are called vergences. A tropia is a manifest deviation of the visual axes. A tendency to deviation of the visual axes held in check by the fusion mechanism is a phoria. See Figure 2 for these and additional terms.
In agonist-antagonist relationships, the muscles pull in opposite directions, for instance, medial rectus versus lateral rectus. To a substantial degree, vestibular gaze and control of oculomotor function are arranged around these muscles as pairs that control rotation in horizontal, vertical, and torsional directions. Synergists are agonist muscles pulling in the same direction. Muscles often are synergists for one direction, such as the superior rectus and inferior oblique for supraduction, while at the same time acting as antagonists for their horizontal and torsional vectors. GLOBE AND ORBITAL AXES The eye is a sphere rotating around three orbital axes: vertical rotation around the horizontal (x) axis, cyclorotation around the anterior-posterior (AP) or y, axis, and horizontal rotation around the vertical (z) axis. The eye has a similar set of axes, which rotate with the eye (Fig. 3). The study by Howard and Templeton provides further description of axis systems.1 The eye and its center of rotation can also be translated by small amounts in other directions: medial to lateral, up to down, and inward to outward.
POSITIONS OF THE EYE The global axes can be compared with the orbital axes in various gaze positions by marking a cross on the front of the cornea to tell how the eye is oriented (Fig. 4).
Primary Position In this position, the two sets of axes, global and orbital, coincide exactly. The geometric AP axis of the eye is normally close to the visual axis and the latter is taken as the y axis. An example is a soldier standing at attention with his eyes straight ahead on the horizon: the eyes in this position approximate the primary position. Secondary Positions These positions rotate around the horizontal or vertical axis only. Movement of any amount vertically straight upward or downward leaves the horizontal (x) axis in its same position and tilts the vertical (z) and visual (y) axes in the vertical plane. A similar situation occurs in purely horizontal rotation away from the primary position. No rotation occurs around the y axis. Tertiary Positions All other positions are termed tertiary positions. If the right eye is turned obliquely up to the right, the horizontal and vertical axes of the eye now no longer stay parallel to the vertical and horizontal axes of the orbit. They tilt relative to the vertical meridian that exists in the new position. This is called cyclorotation or torsion. The eye has rotated around all three axes, including its line of sight, the y axis. DONDER'S LAW AND LISTING'S LAW Donders found that for any gaze position, there is a predictable amount of torsion, and that this is independent of how the eye travels to that gaze position.2 The amount of torsion increases with increased movement of gaze from the primary position. For an oblique position of 10 degrees vertical and 10 degrees horizontal, there is 1 degree of torsion, for 20 degrees vertical and horizontal, 3 degrees of torsion, for 30 degrees, 8 degrees ; for 40 degrees, 15. Listing proposed (and Von Helmholtz formulated and verified) a clever way to consider the torsions that Donders described.3 The image is that of a vertical plane cutting the eye into front and back halves going right through the center of rotation at the equator (see Fig. 3). Next imagine a rod attached to the center of this equatorial plane (called Listing's plane) so that it can spin around like a hand on a clock. This rod is the axis of rotation for the eye. For an eye position straight upward, this axis is placed horizontally from the 3- to the 9-o'clock positions. For a rotation obliquely, this axis is placed at an oblique axis, say 10:30 to 4:30 positions. The advantage is that only two data are needed to describe the eye position instead of three: one, the orientation of the rotation axis, and two, how far the eye rotated in that direction. The torsion that is required to be added in a triaxial system turns out to be automatically corrected using Listing's system. Listing's law has been tested under a variety of circumstances and shown to be correct for vertical and horizontal movements in the frontal plane with the head erect. Listing's law does cease to be demonstrable in abnormal innervations causing restrictions to movement and also for normal convergence positions; there is about 1 degree of excyclophoria for each 4 degrees of convergence. The triaxial system is no problem for modern computers; all serious modeling of eye movements is currently performed using the triaxial scheme. Clinicians think in terms of horizontal, vertical, and cyclotorsional effects of the muscles in a system of three axes. Moreover, the vestibular system driving many eye movements is also organized into vertical, horizontal, and torsional subsystems. But Listing's concept is more than a clever way to think about normal eye rotations and turns out to have some basis in anatomy. Nakayama conceived of Listing's plane as an elastic membrane with the eye suspended in it (Fig. 5).4 If the eye is pulled in any direction, it obeys Listing's law. Anatomically, there is a matrix of fatty fibromuscular tissue suspending the eye and the anterior third of the muscles in the orbit and attached to the orbit walls. This is very like the eye suspended in a foam rubber layer several millimeters in thickness that acts like the membrane of Nakayama. The eye is thus somewhat mechanically constrained. During normal large saccadic movements accompanied by strong head rotation, transient torsional deviations up to 25 degrees have been found,5 showing that this mechanical restraint is only partial. In addition, the eye muscles are programmed to have a certain particular set of pulls for each gaze position. Large deviations from Listing's law occur with non-paralytic brainstem lesions altering the innervation program. So Donders' law is also confirmed by eye muscle innervations.
POSITION OF REST The eye positions of orthophoric, normal individuals under deep anesthesia with curare paralysis are probably the closest approximation to a true position of rest. De Groot and coworkers found an exotropia of 2.25 degrees for each eye in young adults, which increased with age.6 This is in accord with the estimate of most clinicians. In newborns whose eyes are straight when awake, the visual axes are commonly divergent up to 35 degrees in deep sleep, which become progressively straighter within only a few weeks.7 The position of the eyes under anesthesia in strabismus cases helps to show anatomic vertical, horizontal, or torsional factors underlying the alignment disorder. Differences in waking eye position from those while asleep indicate innervational factors. In general, esotropic cases are less esotropic, showing that innervational factors are dominant, and exotropia cases are about the same, showing that anatomic position is the major factor. Difference between the position of the two eyes shows the effect of unequal anatomic factors; rotation of the fundus structures indicate torsional factors. |
| ACTION OF MUSCLES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| The pull of a muscle on the eye is determined by (1) the size of the muscle (cross-section, primarily), (2) the direction it is pulling, (3) the
innervation to the muscle, and (4) the mechanical characteristics
of the muscle. SIZE Cross-sectional areas of the extraocular muscles in square millimeters from Volkmann and Nakagawa's measurements appear in Table 1.8,9
TABLE 1. Eye Muscle Area, Length, and Innervation
COMMENTS
LENGTH The extraocular muscles are from 32 to 40 mm in length (see Table 1). Inasmuch as each 1.0 mm on the surface of the eye corresponds to 4.5 to 5 degrees of rotation, the normal amplitude of eye rotation of 45 to 50 degrees each way from the primary position requires 10 mm change of length of the muscle in each direction. This represents a contraction of 25% to 30% and an extension of 25% to 30% from the normal resting length of the muscle, nearly optimal excursions for linear performance. Sacrifice of muscle length during eye muscle operations can reduce the amplitude of eye rotation. Muscle length is not proportional to eye size, so that large myopic eyes rotate less and small microphthalmic eyes rotate farther than normal. DIRECTION OF MUSCLE PULL Muscle attachments and directions of pull (Fig. 6) are defined as follows:
Origin is the point of muscle attachment to the bony orbit. Muscle plane. The origin, functional insertion, and center of rotation establish an imaginary plane through which the muscle pulls to move the globe (see Fig. 6). Muscle axis of rotation is perpendicular to the muscle plane. The individual muscle pulling on the eye rotates the globe around this axis through the center of rotation. For the horizontal recti, it coincides with the vertical axis of the globe when the eye is in the primary position. For other muscles, it is oriented at various angles established by their coordinates of origin and insertion (see Table 1, Fig. 7).
The forces of muscle contraction and relaxation pull on the eye according to the muscle plane established by the origin, functional insertion, and center of rotation. Clinical strabismus patterns due to anatomic variation of this anatomy, which can be shown on CT or MRI scans, are not rare. For more detailed measurements of arc of contact, exact point of origin, and so forth, see Tables 1 and 2.
TABLE 2. Coordinates of Origin and Insertion of Ocular Muscles*
*Origin and insertion coordinates are expressed in millimeter distances from the center of the globe. Thus, for example, to find the origin of the lateral rectus, we move nasally 13 mm, backward in the orbit 34 mm, and superiorly in the orbit 0.6 mm. To find the insertion of the lateral rectus in the orbit relative to the center of the globe, we move 10.08 mm temporally, 6.5 mm anteriorly; this establishes the center of the insertion point. Actions from the primary position indicate the percentage of the muscle's effort that goes into rotating the eye around each of its three axes. <sd>Values for anatomic coordinates are those of Volkmann AW, summarized in von Helmholtz H: Physiological Optics. (Southall JPC, ed. and Trause.) 3rd ed. New York: Dover Books, 1962.
PRIMARY AND SECONDARY ACTIONS OF MUSCLES One scheme is to assign rotation around each of the axes as a major or minor function of muscles:
Another helpful concept of how each muscle acts from the primary position is to show what would happen if you plotted the direction of your fovea on a wall while each muscle individually pulled the eye in its muscle plane (Fig. 8).
MUSCLE ACTION FOR POSITIONS AWAY FROM THE PRIMARY POSITION When the eye moves to new positions, the orbit axes stay fixed and do not move. The eye carries its axes and the muscle insertions along to the new position with it. The action of each muscle on the eye changes because the eye axes are now in different positions. Figure 9 shows the effect that each muscle pair would have if it were the only one pulling. This graph is like that in Figure 8 but involves other gaze positions in addition to the primary position. The horizontal recti are considered as starting from various positions of vertical gaze. There is a minimal change of effect; they remain as horizontal movers. The effect of the oblique and rectus muscles is considered starting from various positions in the horizontal plane. The vertical rectus muscles have a nearly pure vertical effect when the eye is in abduction, but increasing torsional and horizontal effect as the eye moves into adduction. For the obliques, there is almost purely vertical action in extreme adduction and almost purely torsional effect in extreme abduction. The superior and inferior rectus muscles are quite symmetric, whereas the superior and inferior oblique are not quite symmetric, as a result of the long arc of contact of the inferior oblique.
STABILITY OF MUSCLE PLANES IN THE ORBIT The anatomic muscle insertions on the globe are carried along by rotation of the eye to new positions. What about the functional origins and insertions: are they moved to the same degree as the anatomic insertions? For example, in the classic geometric analyses in Figures 8 and 9, the muscles are supposed to behave as if they were a single string connecting the origin and center of insertion and as if the muscles could slip sideways over the globe.15,16 Four factors alter this: (1) first is the width and geometry of the insertion (Fig. 10). The extraocular muscle insertions are all convex at their insertional end; (2) they are all approximately 9 to 10 mm wide; (3) the muscle almost bisects the center of rotation of the globe on its way to the insertion; and (4) these insertions are all approximately 5 to 6 mm in front of the center of rotation (inferior oblique excepted).
The practical effect of this on, for instance, the medial rectus, is to slack off the upper fibers during upward gaze and transfer the effective tension generated by the muscle from the center of the muscle to the lower fibers. Similarly, in downward gaze, muscle tension is transferred to the upper fibers, and the lower border of the muscle is slack (Fig. 11A). Were this not true, the situation would be as shown in Figure 11B: the medial rectus would become an elevator in upward gaze and a depressor in downward gaze. Similar figures show the stabilizing effect of a wide insertion on the line of pull of oblique and vertical rectus muscles. Von Helmholtz first described this attribute of the width of the extraocular muscles tending to hold the direction of pull of the muscle stable in the orbit, regardless of eye position.
MUSCLE PULLEYS The trochlea (pulley) of the superior oblique constrains the tendon and changes its direction of pull so that a new origin is created. Less dramatic accumulations of fibrous orbital tissue surround the rectus muscles just behind the equator and extend to the orbit holding it to some degree to the orbit wall (Fig. 12). These tissues also act to limit sideslip in the rectus muscle and to limit the surgical effect of rectus muscle transposition operations in which the insertion is moved laterally. They bias the origin as the trochlea does, but to a much lesser degree, thus acting as “soft pulley” (Fig. 13). such displacement occurs in strabismus disorders, but it is not always clear whether the displaced muscle is taking the pulley with it or vice versa. These tissues have long been known to contain smooth muscle fibers.17 Innervation to these structures and their functional significance is a current topic of investigation.
MUSCLE STIFFNESS Imagine that the medial rectus consisted only of two stiff chains. Then, when the eye rotated upward, the smallest bit of slack created by relaxation at the upper border of the medial and lateral muscle totally relaxes tension and transfers it to the lower border. Clearly, this jerkiness would be unsatisfactory, and the smooth compliant nature of the extraocular muscle and its convex anterior insertion are factors that combine to transfer this force easily and smoothly from one side of the muscle to the other. On the contrary, if the muscle were extremely flexible, like a wide elastic band, then relaxation on one side would have very little effect on the transfer of tension along the muscle insertion. In fact, the stiffness of the muscle, about 0.25 to 0.5 g per degree, seems exactly adapted. In awake patients, when the upper part of the medial rectus insertion is cut away from the globe except for 2 mm at the lower end of the insertion, the cut muscle retracts, making an angle of about 45 degrees with the original insertion. When the patient rotates his eye superiorly, the cut superior fibers fall back almost exactly onto the insertion, an indication that the inferior fibers are taking almost the entire strain. Thus, as the eye carries the medial rectus insertion up, the force moves down, keeping its pull horizontal on the globe and horizontal in the orbit. SIDESLIP OF MUSCLES OVER THE GLOBE The intermuscular membrane stabilizes the anterior portion of the rectus muscles from the equator forward, preventing each muscle from slipping sideways. In Figure 14, the path of the lateral rectus in gaze nasally and upward is indicated, assuming the muscle took the shortest path from origin to center of insertion. This extreme upward path is not taken, but a course nearly over the lateral meridian of the eye is maintained by the intermuscular membrane. If the intermuscular membrane is cut away at the time of surgery, the horizontal muscle slips about 2 mm vertically during vertical movements. A second factor holding the rectus muscle from slipping sideways is the adhesion or “foot plate” that attaches the global surface of the muscle to the sclera and extends some 4 to 5 mm posterior to the insertion. Abnormal vertical eye movements from such sideslip of horizontal can occur in strabismus disorders in which high forces gradually tear and obliterate the intermuscular membrane (Duane's syndrome), and in high myopia in which expansion of the globe, usually in the upper temporal area, stretches the intermuscular membrane and pushes the lateral rectus downward. These disorders can be treated by fixing the muscle to the sclera at the equator to prevent sideslip.18,19 The superior oblique tendon has a very short length and arc of contact, and here sideslip is not a significant factor. The inferior oblique has a very long arc of contact. Indeed, the necessary length of muscle to allow extension and contraction is provided by the coiling of the inferior oblique muscle around the globe for a long distance. The ligament of Lockwood, at the crossing of the inferior oblique and inferior rectus muscles, acts to prevent A-P slip of the inferior oblique, just as the intermuscular membrane acts in terms of the rectus muscle (Fig. 15). Eye muscles imaged on MRI scans had only small sideslip when subjects fixated in various directions.20
COHESIVENESS OF THE MUSCLE The belly of the muscle is readily split longitudinally because it contains little transverse fascial tissue, but the anterior muscle is cohesive within itself to prevent separation because otherwise, the fibers of the lateral rectus muscle would splay out almost 18 mm wide in extreme gaze into elevation and adduction. Thus, the anterior muscles, their surrounding Tenon's fascia, and the intermuscular membranes form a continuous stabilizing band or cap around the globe extending from the muscle insertions anteriorly back to the equator. The muscle “pulley” tissue anchoring the muscles to the orbit adds to this. FIELD OF ACTION OF MUSCLES Even though all these muscles have some effect on the eye in every gaze position, each pulls preferentially in a specific direction, called its field of action. Torsion is not usually considered, only horizontal and vertical actions. The field of action is established by two considerations: geometry and innervation. GEOMETRY We have seen in our analysis that the lateral rectus pulls toward abduction almost exclusively. That is its field of action. The medial rectus pulls toward adduction almost exclusively. That is its field of action. For vertical gaze such a simple arrangement is not present, for a combination of muscle actions exists. In 23 degrees of abduction, the superior rectus is a pure rotator around the horizontal axis of the adducted eye. This is its field of vertical action for clinical testing. If the eye rotates well vertically in this position, it must be due to a normal superior rectus. Here, the inferior oblique muscle contributes little vertical movement. In adduction, the oblique becomes an increasing elevator, but the superior rectus remains a substantial elevator even in adduction because of its angle of insertion and its greater cross-sectional area. Thus, elevation in adduction is a combination of inferior oblique and superior rectus activity. Nevertheless, vertical contribution of the oblique can be assessed clinically by comparing elevation in abduction, in which it has virtually no effect on elevation, with elevation in adduction in which it contributed 45% to 50% of elevation (Fig. 16). The superior oblique and the inferior rectus muscles have the same relationship in infraduction. The inferior rectus is virtually the sole infraductor in the abducted gaze positions, and both the superior oblique and the inferior rectus contribute as gaze is moved toward adduction.
INNERVATION TO HORIZONTAL MUSCLES In addition to the mechanics, changes in the innervation to the muscles in various gaze directions establish what they do; this might be thought of as field of activation. For abduction, innervation progressively increases to the lateral rectus as the eye abducts from the primary position. This is true whether it starts from the primary position, or whether the eye starts from a position of slight elevation or depression: the program of innervation of the lateral rectus appears to be the same. Similarly, the medial rectus increases activity with all attempts to adduct the eye, whether the eye starts in the primary position, in moderate supraduction, or moderate infraduction. INNERVATION TO VERTICAL MUSCLES The elevators of the eye, the superior rectus and the inferior oblique muscles, probably receive equal innervation increments during supraduction attempts, and this is true whether the eye is straight ahead, abducted, or adducted. That is, if one establishes a horizontal line 30 degrees above the primary position, whether the eye looked at the adduction end, the middle of the line, or the abduction end, any individual vertical muscle has the same innervation. The same applies for infraduction involving the superior oblique and the inferior rectus. Thus, it must follow that the oblique muscles and the rectus muscles establish their field of vertical action primarily on the basis of mechanics, and they do not separate themselves one from another on the basis of differences in innervation reaching them in adduction versus abduction. We occasionally find a motor unit within, say, the inferior rectus that changes its innervation in the downgaze plane slightly, increasing slightly in abduction, but decreasing with adduction. However, just the reverse of this may be seen in another patient. Consequently, minor variations from the general rule occur. Perhaps these variations act to correct differences in anatomy from one person to another. We know oblique muscle planes are at 30 degrees to the visual axis in one person and 50 degrees in another; perhaps these variations represent individual innervational adjustments that develop during infancy and visual development to achieve concomitance. These variations may have been the basis of the anecdotal reports of difference in vertical muscle innervation in abduction vs abduction.21 Data on the innervational change of vertically acting eye muscles with gaze are few and a careful systematic study remains to be done. For vertical fusion movements, evidence from the torsional position of the eye indicates that the oblique muscles are the primary movers, not the vertical rectus muscles,22,23 although electromyographic (EMG) studies remain to be done. Vertical supraduction during forced blinking (Bell's phenomenon) appears to be carried out primarily by the oblique muscles. AMPLITUDE OF ROTATION OF THE EYE In normal children, the eye can rotate from the primary position about 45 to 50 degrees horizontally and downward and about 40 to 45 degrees upward. This 45 to 50 degrees of movement requires about 10 mm of contraction and 10 mm of relaxation from the primary position (4.8 degrees of rotation equals 1 mm of distance on the sclera). Supraduction diminishes with age. It is reduced a bit even by age 25 and averages only 16 degrees of supraduction at age 80. Other directions of gaze persist better. Exercise helps.24 Donders pointed out that the eyes of myopic people rotate less than this.2 The center of rotation is more posterior in myopic people, effectively increasing the radius of the eye as it rotates and thus giving less rotation for each millimeter of muscle shortening. On the contrary, microphthalmic eyes can often turn more—up to 70 degrees abduction! |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| FINE STRUCTURE OF MUSCLES | ||||||
|
We know from human EMG study that eye muscles are constantly active when awake; therefore, they need much stamina. Eye position can be accurately maintained; this requires fine control. Rapid eye movements are possible: this requires high speed of muscle contraction. These attributes—precision, speed, and stamina—are physiologic properties of a motor unit reflected in the structure of the muscle fibers that comprise it. Using various histologic criteria, anatomists are able to subdivide at least five types of muscle fibers in the extraocular muscles.25 MUSCLE LAYERS Almost all investigators find that the extraocular muscles of mammals are divided into two layers to some extent: a global or central layer, next to the eye, and a superficial or orbital layer confined to the posterior two thirds of the rectus muscles and less evident in oblique muscles. This layering is much less obvious in humans than lower species (Fig. 17). The orbital layer has a high capillary density and generally contains small fibers. Scott and Collins confirmed that, in humans, fibers that are active constantly for fixation near the primary position are predominantly in this layer.26 By the classification of Alvarado and Van Horn in cat, the orbital layer contains two fiber types.27 Both are relatively small, rich in mitochondria, and contain some lipid vacuoles. About 60% to 70% of the cells are singly innervated with good sarcoplasmic reticulum content, which allows rapid calcium ion changes with each contraction, and about 30% to 40% are multiply innervated slower fibers.
The global layer contains one type of multiply innervated fiber and three types of single innervated fibers of varying size, mitochondrial supply, and sarcoplasmic reticulum content. Type 1 is a large, pale, relatively mitochondria-free type rich in endoplasmic reticulum. This should be a very fast but readily fatigued fiber, good for saccades and for short periods of extreme gaze. These fibers constitute about 30% to 40% of the total number, but they occupy about 60% of the core area and thus contribute importantly in terms of strong but temporary force production. Types 2 and 3 are progressively smaller and contain increasing amounts of mitochondria and probably decreasing amounts of endoplasmic reticulum. These would be more fatigue resistant and slower in response than those that contain a great deal of cytoplasmic reticulum. MUSCLE FIBER ORIENTATION The muscle fibers are mostly parallel, but some side-to-side and end-to-side junctions of muscle fibers exist, creating a network within the global layer. Many fibers thus terminate before the end of the muscle; a cross section at the center shows more fibers than cross sections near either end. Oh and Demer have recently counted the fibers in the rectus muscles of monkeys and humans and confirm this restriction of the orbital layer to the posterior two thirds of the muscle.28 Surprising was the finding of insertion of some of these orbital fibers onto the fibromuscular tissue (“pulley”) in Tenon's fascia near the anterior one third of the muscle. FASCIA IN MUSCLES The endomysium surrounding these fibers contains substantial elastic tissue. The perimysium surrounding groups of muscle fibers contains more collagen fibers. Within this area run the small vessels and nerves to the muscle. These collagen fibers run along the length of the muscle; thus, their shortening by inflammation, scar or lack of being stretched by antagonist contraction (e.g., in paralysis) results in stiffening and restriction of eye movement, a common clinical problem. MUSCLE CONTRACTION In Figure 18, the muscle is diagrammatically dissected into its components. The heavy filaments are myosin; the thin filaments, a double helix of actin with additional proteins, tropomyosin, and troponin. The sliding of these filaments past one another provides length change, especially apparent in Figure 19. As thick and thin filaments of the muscle fiber slide past one another, the bridges between these filaments maintain the strength of the muscle. If there were many crossbridges, there would be more force, and if there were fewer crossbridges, there would be less force, as seen in isometric testing. In Figure 20, one can see that as the muscle is normally stretched, the number of cross bridges being effectively used maximumizes and then gradually diminishes as further stretching occurs. Unlike many muscles that work over a large range, extraocular muscles work almost entirely in the region from 1 to 2.2; that is, the rather linear slope to the left of the peak of tension. To work within this range, sarcomeres of muscles cannot be greatly stretched or compressed from their normal length of about 2.3 μm. When muscles are maintained at a stretched or shortened length for weeks or months, they respond by adding or removing sarcomeres to regain this length of 2.3 μm. Muscles so shortened become stiff also and cannot be distinguished mechanically from fascial or fibrotic contraction.29
DIFFERENCES IN TENSION Both singly and multiply innervated types of eye muscle fibers are composed of thick and thin filaments of about the same length. Thus, it is not surprising that they give about the same total force for each cross-sectional area.30 THE T SYSTEM How can a wave of depolarization sweep through an eye muscle and cause a twitch in 2 msec? Invaginations of the muscle membrane, the sarcolemma, extend into the muscle fiber in a direction transverse (t) to the axis of the fibrils, carrying the wave of polarization into the muscle itself. The sarcoplasmic reticulum that stores calcium necessary for activation is associated directly with these transverse tubules. Much T-system and sarcoplasmic reticulum is present in eye muscles to allow very rapid contraction frequencies up to 400 Hz. MITOCHONDRIA Mitochondria provide power to the muscle by oxidative phosphorylation. Because muscle contraction is powered by dephosphorylation of adenosine triphosphate, mitochondria are one source of energy. Thus, the more mitochondria present, the more power and stamina are provided. The extraocular muscles have an extremely high content of oxidative enzymes associated with the mitochondria. SINGLE AND MULTIPLE INNERVATION In certain eye muscle fibers, the filaments are separated into bundles. Obvious under light microscopy, this fibrillar pattern (Fibrillenstruktur) is generally associated with rapid, twitch-type contraction. A horizontal view of such a fiber (Fig. 21) reveals the extensive mitochondrial involvement and the differentiation into small bundles. Most of these fibers have single nerve innervation by only one motor endplate. Such a fiber is adapted for rapid, short-term use. In other fibers, the fibrils are not divided much into separate bundles, giving a rather uniform field of distribution (Felderstruktur). Some of these muscle fibers contract only in local areas of the muscle by local innervation around multiple nerve endings along the fiber, without an overall depolarization and twitch. In Figure 22, such a fiber is seen in cross section, again emphasizing the lack of separation into myofibrils. Such fibers would be less capable of high frequence contraction but more capable of slow, steady, stamina-oriented tasks.
BLOOD FLOW AND FATIGUE Blood flow in the extraocular muscles must be exceedingly high to account for the rapid metabolism. Indeed, average blood flow per gram of extraocular muscles proportionally to that of other skeletal muscles and was second only to myocardium.31 Eye muscles are very resistant to fatigue under laboratory conditions. Extreme gaze to one side for several minutes, however, gives rise to unstable fixation in humans (end-gaze nystagmus). This is unequal in the two eyes, so it appears to be a fatigue of the muscles or motor units rather than of gaze function. CHANGES IN EXTRAOCULAR MUSCLE WITH AGE AND DISEASE Miller found alterations in staining characteristics, occasionally degenerating nerve fibers, and disturbance of the orderly fiber alignment and direction of human muscles after age 30.32 With age, the collagen fibers within the muscle itself increased. As motor nerve fibers drop out with neuron death, the remaining nerve fibers send sprouts to form new neuromuscular endings on the denervated muscle fibers. This process preserves muscle strength with aging. A similar sprouting in partial nerve damage leads to prolonged recovery with large motor units. The different types of muscle fiber are probably susceptible to diseases at varying rates. For example, muscular dystrophies associated with mitochondrial abnormalities should especially involve extraocular muscles. Cogan and colleagues have proposed a susceptibility difference seen also in myasthenia gravis.33 |
| THE MOTOR UNIT | ||
|
The motor neuron cell body, axon fibers, and muscle fibers that they supply are collectively called a motor unit.34 In skeletal muscles, the muscle fibers comprising a motor unit are spread widely about in the muscle, perhaps to even out mechanical pull. In eye muscles, however, the muscle fibers in a single unit are probably in rather close bundles.35 Tiny movements of a recording electrode within an eye muscle markedly reduce recorded activity of a particular unit, a finding inconsistent with a very “spread-out” distribution. Much of our understanding of motor unit physiology comes through EMG. When the usual EMG electrode records muscle activity, it picks up extracellular signals of twitch-type muscle fibers. Changes in muscle membrane potential that remain local and are not propagated might escape detection; we might thus fail to understand the function of some multi-innervated fibers. However, investigators find a pattern of activity in the ocular motor nuclei (where all these motor units are represented) that correlates well with the EMG pattern found in humans.36,37 The number of muscle fibers supplied by any particular nerve fiber varies; one nerve fiber may supply as many as 140 skeletal muscle fibers. On the average in human extraocular muscles, the ratio has been estimated to be about one nerve fiber to six muscle fibers. Distribution of the nerve fiber sizes in nerves to human extraocular muscles is a bimodal (Fig. 23).38 Muehlendyck has calculated the innervation ratio of the larger muscle fibers and that of the smaller muscle fibers on the basis of the assumption that larger nerve fibers go to the larger muscle fibers and small nerve fibers to the small muscle fibers.39 This ratio is one nerve fiber for each three or four small muscle fibers, good for fine tuning of position, and one nerve fiber to ten or more layer muscle fibers, good to provide the force for saccades.
It would be advantageous to employ physically small motor units to grade with accuracy the amount of contraction or relaxation around the primary position. On the contrary, it would be greatly advantageous for a rapid saccadic eye movement to recruit a motor unit large in size (not only is the number of fibers in the fast unit greater, but their size is also much larger), and thus tension would rise rapidly for the saccadic eye movement. On the basis of these considerations, Robinson's scheme indicates the possible participation of motor units of different muscle fiber anatomy as the eye moves from out of the field of action of the particular muscle (“off”) into the field of action of the muscle (“on”) (Fig. 24).40 This is consistent with the data found in humans as reported by Scott and Collins.41
|
| PURPOSE AND TYPES OF EYE MOVEMENTS |
|
The successful use of vision comes, in part, from being able to control gaze, that is the position in space to which the eyes are pointed. Gaze results from the sum of body, head-on-body, and eye-in-head movement. Primates, and humans in particular, show great variability in the relative mix of body, head, and eye movement used to establish gaze. A normal person told not to move the head makes perfectly good gaze changes to targets within the orbital range using eye movement only. In contrast, gaze control in nonhumans is more stereotypical and almost always involves combined eye and head movement. The human oculomotor system shares, to some degree, gaze-controlling strategies with the most primitive vertebrate forms and thus reflects a long evolutionary history. A handful of interacting oculomotor subsystems exists, each with its own purpose. The vestibular system compensates for movements of the head (the vestibulo-ocular reflex or VOR). The optokinetic system compensates for motion of the visual surround. The smooth pursuit system, an additional visual tracking system, moves the eyes to track a small visible target smoothly. The saccadic system abruptly moves the eyes from one point in the orbit to another. The vergence system aligns the visual axes of the eyes on the target as the target's distance changes. The fixation system holds the eye on a stationary target. Natural eye movement is a simultaneous integration of these basic types. The smooth pursuit, vestibular, optokinetic and saccadic systems produce conjugate eye movements: both eyes move similarly. The vergence system, in contrast, produces disjunctive eye movements: each eye moves differently. Assessment of eye movement behavior would be simple if, for each oculomotor subsystems, a strict relation could be made between an eye movement type and its adequate stimulus. Unfortunately, eye movements result from a complex interaction of physical stimuli, which often activate multiple subsystems, and unique psychological factors, which modulate responses to the same stimulus. Furthermore, no physical stimulus is necessary to make some types of eye movements. Saccades, for example can be executed in a goal-directed fashion voluntarily in the dark to imagined targets; smooth pursuit, on the contrary, cannot be executed without a moving target by most. The psychological factors involved are often ill-defined and beyond rigorous control. Not too surprisingly then, in the clinic, assessing intrinsic oculomotor capability poses a formidable challenge. Some patients may have difficulty in understanding directions, others may have difficulty concentrating on the task at hand and others may be less willing to cooperate. In all these particulars, children are especially troublesome.
|
| EYE MOVEMENT PSYCHOPHYSICS | ||||||
|
The purpose of this section is to survey overall oculomotor capacity ignorant of the underlying biologic machine. VESTIBULO-OCULAR REFLEX Except for those virtually eyeless animals, all vertebrates possess the standard six extraocular muscles, whether lateral or frontal eyed, developed for roles as predator or prey.42 They all make reflexive, compensatory eye movements in response to a movement of the head. All three sorts of natural head movement are more or less compensated: head rotation activates the angular VOR (AVOR); head translation activates the linear VOR (LVOR); and head tilt in a coronal plane activates the torsional VOR (TVOR). Associated eye movements are compensatory because, for example, to a rightward head movement, the eyes move reflexively leftward in an attempt to steady the visual image on the retina. There are numerous variations on this theme. Usually, VOR performance is better when combined with visual cues. This reflex response is referred to as visually enhanced VOR (VVOR). When the result of a deliberate head movement, the VOR is called active, or passive when the result of external forces moving the head. Active and passive VORs may differ given that the former can be influenced simultaneously by the cervico-ocular reflex and perhaps by internal command signals (efference copy), but the effect of either in normals appears small and is not usually considered.43,44 Active or passive head movement can be either transient, that is, the head moves from one steady position (or velocity) to another as, for example, one might orient toward something far to one side, or oscillatory as, for example, one might track an insect flying nearby. Additionally, the head (and body) can be passively rotated. Such continuous rotation in one direction is unnatural for humans but not necessarily so for fish swimming in tight circles or being carried by swirling currents. Vestibular Stimulation in Darkness The rationale behind using sinusoidal stimuli is that theoretically, any more complicated head movement can be represented by a sum of sinusoidals, the so-called Fourier expansion, and so if superposition* would hold for the VOR, the response to any complex stimulus can be predicted. Indeed, superposition has been shown to hold for the VOR in darkness.45 Figure 25 depicts the eye movements measured during large-amplitude sinusoidal head rotation in darkness. As shown in trace E of that figure, segments of compensatory eye movement (slow phases) are interrupted from time to time by abrupt resetting eye movements (quick phases) in the opposite direction. The composite behavior is called vestibular nystagmus. (Nystagmus derives from the Greek word meaning “to doze,” which is in this sense extended to eye movements because of the similarity to the characteristic diphasic head bobbing seen as one dozes while sitting upright.) If X1, X2, X3, … are different inputs to system corresponding to outputs Y1, Y2, Y3, . . , then for a system with the superposition property and input a1 X1 + a2 X2 + a3 X3 + … , the output would be a1 Y1 + a2 Y2 + a3 Y3 + … , in which unit a1 represents a constant scalar. Superposition is a necessary and sufficient condition for a system to be called linear. Linearity does not imply at all that inputs and outputs.
VOR efficacy can be assessed using various methods. A perfectly compensatory VOR would have the eye rotate in the orbit by an amount equal to, but opposite, the head movement: images of visual targets would be locked on the retina. Because of the ensuing nystagmus, comparing eye excursion, as in trace E, with head excursion would provide a poor measure. From eye position data, cumulative slow phase position can be derived by first extracting the quick phases.46 A simpler method compares eye velocity (E) to head velocity (H). By comparing traces (ignoring those spikes arising from the quick phases) and H, for example, the compensatory nature of the VOR is easily appreciated (see Fig. 25). If the eye was on target before the head started moving, then a system designed to match eye velocity to head velocity perfectly would also keep the eye on target during head movement. Thus, a measure based on velocity seems reasonable and is widely used. At a given stimulus frequency and amplitude, two metrics, VOR gain and phase, characterize eye movement. Most authors calculate gain by |E|/|H| where |E| and |H| are the magnitude of eye velocity and head velocity, respectively. A perfectly compensatory VOR has a gain of 1. For sinusoidal stimuli, phase measures the relative shift between the E and H signals in degrees. A perfectly compensatory VOR has a phase of 180 degrees. Some authors report phase with respect to 180 degrees (such as Φ in Fig. 25). Phase can be estimated by noting corresponding points on the E and H traces or by direct calculation using mathematic approaches, such as that provided by Fourier analysis. A Bode plot summarizes, in two graphs, the VOR gain and phase measurements plotted against frequency. During small-amplitude oscillation in the dark, the occurrence of quick phases depends on the subject's instructions. Quick phases were absent when study subjects were asked to imagine a stationary target but occurred often when these people performed mental arithmetic.47 Quick phases, therefore, are not intrinsically linked to vestibular stimulation. Other aspects of the VOR are revealed by rotating a normal, upright human subject continuously at a constant velocity about an earth-vertical axis in darkness. This elicits an initially brisk vestibular nystagmus (Fig. 26A). As rotation progresses, the slow phase velocity of the per-rotatory nystagmus decreases to 0 following a roughly exponential time course (see VN I in Fig. 26A). The exponential time constant, Tvor, measures about 10–15 seconds. In many subjects a small-amplitude nystagmus builds and decays anew with anticompensatory slow phases (see VN II in Fig. 26A). When rotation ceases, postrotatory nystagmus starts with slow phases directed oppositely to the previous, per-rotatory slow phases (see Fig. 26B). Slow phase velocity during postrotatory nystagmus follows a time course that looks much like the mirror image of the per-rotatory pattern. Many subjects demonstrate a late reversed postrotatory nystagmus, as well.
Efficiency of the VOR Of all oculomotor subsystems, the VOR responds most quickly to stimulation: eye movement commences within 14 msec after head movement.48 VOR gain is rarely unity and unfortunately, VOR gain not only depends on stimulus parameters but also the subject's mind set. For example, VOR gain in the dark for passive sinusoidal head movement at 0.3 Hz measured 0.94 when the subject was instructed to imagine a stationary target but fell to 0.65 when the subject performed mental arithmetic.47 In alert and motivated normal subjects, VOR gain, in darkness, during high velocity, transient head turns, is near unity to about 350 degrees/sec and does not depend on whether the movement was active or passive.49 With higher head velocity, eye velocity tends to increase (and could exceed 500 degrees/sec), in addition to becoming more variable. Considering that the eyes are set apart and that the axes of eye rotation are not coaxial with the axis of head rotation, to compensate for head movement while the eyes are converged on a near target requires horizontal VOR gain greater than unity to be compensatory, reaching a value near two for targets close to the eye. Such gain increases have been measured.50 This high gain has been shown to depend on convergence rather than accommodation and to decrease with frequency of head shake above 1 or 2 Hz.51 Torsional Vestibulo-Ocular Reflex Rotation of the head about a naso-occipital axis gives rise to a weak torsional VOR presumably mediated by the utricule. Tosional VOR is conjugate and counterrolls the eyes about 20% of head tilt within 30 degrees of the vertical.53 Vestibulo-Ocular Reflex Plasticity If not for the adaptability of the VOR, use of correction spectacles would be impossible. Not only do lenses change the focus of visual images, they likewise change, by virtue of their minimizing or magnifying power, the amount of eye movement required to compensate for head movement. As an exaggerated example, if a subject is fitted with spectacle lenses with × 2 power then a 10-degrees/sec compensatory head movement would require a 20-degrees/sec eye movement in the opposite direction, twice the velocity needed without the lenses. VOR plasticity likely did not come about so that correction lenses could be worn but instead imparted an animal with the ongoing capability of using vision to adjust VOR gain as necessary. VOR Maturation Eye movement recordings suggest that the VOR in infants differs somewhat from the VOR in adults. The VOR time constant in newborns is short, less than 1 second compared with about 10 seconds in adults, approaching adult levels within 3 months after birth.54 OPTOKINETIC SYSTEM Optokinetic eye movements, by definition, are driven by movement in the visual scene. Thus, all oculomotor subsystems except the VOR come into play when tracking a visual target with the head stationary. One of these subsystems, the optokinetic system (OKS) evolved early in vertebrate history in fish55 and supplements the VOR by eliciting compensatory eye movements in response to large-field retinal stimulation, the rationale perhaps being that whenever the images of most everything visible move within a “stationary” world, then most likely the eyes moved in space rather than the other way around. To a suddenly presented stimulus such as a full visual field of horizontally translating vertical stripes, the optokinetic response is the rapid onset of optokinetic nystagmus (OKN) with slow phases in the direction of stripe motion (Fig. 26C). In humans, peak slow phase eye velocity is reached during the first slow phase.56 As long as the stimulation continues, OKN continues unabated. The ratio of slow phase velocity to stimulus velocity defines OKN gain, which is close to unity for stimulus velocity up to 60 to 90 degrees/sec. Instructing subjects to pick out and follow stripes (look mode) results in large amplitude, low frequency (more than 40 degrees at about 1 Hz) nystagmus while instructing subjects to stare straight ahead results in small amplitude, high frequency (less than 20 degrees at about 2 Hz) nystagmus.57 Without instruction, most subjects naturally adopt the stare mode. If all lights are extinguished during OKN, nystagmus, in most subjects, does not stop entirely but continues as optokinetic after-nystagmus (OKAN) with an attenuated slow phase velocity that slowly decays away in about 1 minute (see Fig. 26C). The initial OKAN slow phase velocity depends not just on the OKN stimulus velocity but also on the OKN stimulus duration; longer duration OKN stimulation (up to 1 minute) leads to higher velocity slow phases during OKAN. The latter property has been called velocity storage.56 Two integrated signal pathways have been postulated to explain OKN and OKAN. The so-called “direct” signal pathway produces the nearly instantaneous, rapid rise of eye velocity at stimulus onset. The so-called “indirect” signal pathway slowly charges the velocity storage element during OKN and discharges the “stored velocity” during OKAN.58 If OKN stimulation is prolonged, OKAN, which beats in the same direction as the OKN, is followed in some subjects by optokinetic after-after nystagmus (OKAAN), which beats in the opposite direction (Fig. 26C). (There is no agreed upon terminology of optokinetic after-nystagmus. Other terms for OKAN include primary OKAN and OKAN I and other terms for OKAAN include secondary OKAN, reversed OKAN, and OKAN II.) OKAAN is thought to reflect OKS habituation.59 Interestingly, labrynthine disease abolishes OKAN when the optokinetic stimulus produced OKN with fast phases toward the affected ear.60 A particularly curious observation is the sensation perceived during full-field optokinetic stimulation. At stimulus onset human subjects report that only the drum is moving but after a short while most subjects report the sensation of slow self rotation in a direction opposite to the drum's rotation, a phenomenon called circular vection. Circular vection builds until the subject is convinced that the drum is stationary and it is the subject who is rotating exclusively. Nothing in the OKN record, however, reflects the development of circular vection. SACCADIC SYSTEM The saccadic system generates all reorienting eye movements. When these eye movements are used to acquire novel visual targets or correct for positioning inaccuracies and drift they are referred to as saccades. The French word saccade means jerk and appropriately describes the eye's behavior. When these movements reset the eye during nystagmus, the resulting phenomena are called quick phases. Physiologically, saccades and naturally induced quick phases are not known to be different.61 Saccades are often called fast or rapid eye movements but this seems poor terminology because the vestibular system can generate “slow” phases of comparable velocity.49 Amplitude Range of Saccadic Eye Movement Normally, saccades can start at any orbital position and go to any other. The smallest voluntary saccade is reported to be about 0.05 degrees.62 The smallest involuntary saccade (termed a microsaccade) measures about two thirds smaller, only about 0.017 degrees.63 In the natural setting, however, eye position errors smaller than about 0.5 degrees may not elicit a saccade at all, despite the detection of such errors by the visual system and the ability of the saccadic system to make tiny saccades.64 Young refers to this as an “indifference threshold.” On average, saccades are much larger than this but are usually less than 15 degrees.65 Saccade Waveform Figure 27 shows the approximate timing of the more common tests used to elicit and study saccades. Each bar in the figure represents the appearance of a small visible light at some position. Each example begins with a subject fixating a small light at position F. In A (step test), the light at F is extinguished and instantaneously the light appears at target position T. The distance between F and T is the step size. Figure 28 depicts a set of normal voluntary horizontal saccades recorded during a step test where the position of T was varied along a horizontal line through F. As seen in Figure 28, horizontal saccades of different sizes are not scale replicas of each other. The early part of the trajectories coincide but larger saccades have longer durations than smaller ones. Not as obvious in Figure 28, larger saccades have higher peak velocities. A plot of average saccadic peak velocity against saccadic amplitude (Fig. 29) reveals a saturating curvilinear function called the saccadic main sequence, a term borrowed from the literature of astronomy. The data for saccades less than 20 degrees have been fit by
θmax = 684 (1 - e-0.1) where max
is peak eye velocity, θmax is saccade amplitude and e
is the base of the natural logarithm ( Tdur = 0.0022Δθ + 0.021 A saccade's step gain is the ratio of the saccade's amplitude to the target step size and is measured at a point in time after any postsaccadic drift has subsided. Saccades that land immediately on target are called orthometric or normometric. Those falling short of the target are called hypometric whereas those going past the target are called hypermetric. Often a saccade reaches a final position after a period of postsaccadic drift. Slow postsaccadic drift is also called a glissade. Fast postsaccadic drift in a direction opposite to that of the original saccade, as seen in Figure 28, lower trace, is often called dynamic overshoot. Dynamic overshoot and slow drift can both occur after the same saccade.69 The mechanism giving rise to dynamic overshoot in small saccades is moot. The observation that the decaying phase of the overshoot fits on the main sequence has led some researchers to suggest the overshoot is saccadic and results from a deliberate effort to generate gaze shifts in the least amount of time.71,72 The report that the overshoot, when found, is almost exclusively observed in the abducting eye69—an apparent violation of Hering's law—led to a computer modeling study showing that overshoot in one eye with no overshoot in the other can be explained simply by mechanical differences of the two orbits, that is, the overshoot arises passively.73 The reaction to a stepped target may not be just a single saccade although it commonly is for small saccades. For large target steps, subjects often make two saccades: an initial primary saccade covering about 90% of the displacement followed by a secondary saccade to the target (see Fig. 28, top four traces). Rarely, some normal subjects require a tertiary saccade to acquire the target. Although any saccade that reduces the error between the current eye position and the target could be called a corrective (or correction) saccade, the term is not usually used in referring to the large primary saccade. That corrective saccades persist in total darkness suggests that the corrective saccade is not driven by actual retinal error but is preprogrammed, generated in anticipation of error after the primary saccade.74 Why the primary saccade is ordinarily hypometric is not known but appears purposeful because when feedback is used to move the target position systematically after the saccade is under way to the position that would be normometric for the primary saccade, the saccadic system, after only a few exposures reduces the amplitude of the primary saccade to, in effect, reestablish the primary hypometric saccade.75 Corrective saccades lie on the main sequence suggesting they are executed using the same machinery as the primary saccades. Saccade Latency and Refractoriness When subjects are repeatedly tested with unpredictable saccadic targets, the distribution of latency between the appearance of the target and the start of the saccade typically is multimodal. Three latency modes are recognized: the shortest peak between 100 and 135 msec, express saccades; a second one between 140 and 180 msec, fast regular saccades, and a less common third peak about 200 msec, slow regular. Saccades with shorter latency are typically considered anticipatory. The relative frequency in each mode depends on the specific saccade test. If the duration of F in Figure 27A is random, the eye, after an average latency interval of about 200 msec makes a saccadic eye movement toward T.76 Many factors influence saccadic latency, some involve the physical properties of the target, others involve cues to predict a target's future movement from its past movement. For random target steps larger than 1 degree, saccadic latency is largely independent of saccade amplitude with only small increases for large (e.g., more than 40 degree) saccades.77 For random target steps less than 1 degree, latency (and its variability) dramatically increases to about 400 msec for a 0.06 to 0.2 degree target step.78 When subjects can anticipate an upcoming saccade, especially its direction, latencies are reduced. In an extreme case in which the target is stepped back and forth between two points repeatedly, subjects predict the target motion and can “track” with almost no latency at all.79 If the light at F is held on after the target appears at T (overlap test, see Fig. 27B), the average saccadic latency is longer than when no overlap exists.81 Alternatively, inserting a short interval of time (100 to 200 msec) between the offset of light at F and the appearance of T (gap test, Fig. 27C), decreases the average saccadic latency of most subjects because the express saccades are favored, even when anticipatory saccades are removed.80 Making target selection harder by presenting T along with other potential targets increases average latency and eliminates express saccades.81 The sequence in Figure 27D can test for short-term memory in the saccadic system. Here the light at T appears transiently whereas F remains visible. The subject is usually instructed to look to the remembered position of T as soon as F goes out. Subjects can be instructed to make prosaccades to the target or antisaccades opposite the target. An antisaccades task tests a subject's ability to override visual grasp reflexes. In the clinic, saccadic latency to visual targets may provide a sensitive indicator of optic neuropathy where, for example, above normal latency has been correlated with afferent conduction loss.82 Oblique Saccades Oblique saccades in humans are normally curved83 with the horizontal and vertical components generally synchronized.84 Curiously, the duration of the orthogonal components usually differs: for saccades smaller than 15 degrees the horizontal and vertical component durations seem to be independent84,85 but for saccades larger than 15 degrees the shorter duration component is stretched toward the longer duration component.84 Rhesus monkeys, in contrast, tend to make straight oblique saccades.86 Saccadic Plasticity Saccades are so fast that visual feedback is not possible during saccade execution to ensure accuracy. Instead, the brain uses postsaccadic visual cues to guide adjustments in the preprogramming of future saccades: both static errors (hypo- or hypermetric saccades) and dynamic errors (excessive postsaccadic drift) can be eliminated.87 Adaptation to static errors can be studied with the sequence in Figure 27E. Here the detection by circuitry of the saccade toward T triggers a second jump of the target to position T'. When T' is sufficiently close to T subjects remain consciously unaware of the second jump despite generation of appropriate corrective saccades. If this test is repeated over and over, the brain gradually adjusts the saccade to approximate the saccade previously made to a target step from F directly to T'. Vision during Saccades As we look around a continuously lit scene we do not sense the smeared retinal image caused by the eye's high velocity during saccades. When scene illumination is confined entirely to the duration of the saccade, however, a smeared image is indeed perceived.88 Experiments wherein patterned visual stimuli were flashed only during saccades have shown that detection thresholds were raised a mere 0.5 log units above the detection threshold when the stimuli were presented at fixation.89 Thus, vision is not blanked during saccades. Other experiments have demonstrated that clear images presented before and after a saccade mask the appreciation of image smear during the saccade.92 SMOOTH PURSUIT SYSTEM When using eye movements only, a normal subject tracks a small moving target with a mixture of smooth pursuit, saccadic, and vergence eye movements. The overall strategy is to maximize acuity by keeping the target close to the fovea while reducing retinal image slip. For a particular subject, the relative mix of smooth and saccadic eye movement to track a target moving on a uniform background depends primarily on target velocity and regularity. The smooth pursuit subsystem (SPS) creates the conjugate smooth pursuit component. SPS gain, the ratio of eye velocity to target velocity, seldom is unity so that as the eye drifts away from the target saccades are triggered to reduce the accumulated error.91 SPS gain decreases with increasing target velocity, increasing target eccentricity with respect to the fovea, decreasing target movement predictability and decreasing attention. SPS gain is also lower when the moving target is viewed against a stationary structured background.90 With an alert subject, as SPS gain decreases for whatever reason, the frequency of catch-up saccades increases, thus keeping the target close to the fovea. Higher SPS gain when tracking predictably as opposed to randomly moving targets hints at a fundamentally complicated system: a simpler control system would depend only on the target's instantaneous kinematics. Further along this same line, the observation that the SPS can be, to some extent and with practice, driven by perception in lieu of retinal image motion along the pursuit direction92,93 has not yet been explored beyond psychophysics and is too often ignored. Reliance on an internal model of target motion probably stems from the somewhat longer time needed by the visual system to process motion cues. Generally, though, voluntary smooth pursuit requires some motion cues, either visual, proprioceptive, or auditory. Nevertheless, target image slip on the retina is considered the primary input to the SPS but constant retinal error can be an adequate stimulus as well.94,95 In primates, the SPS clearly can drive eye movements more powerfully than the OKS because a small target can be easily tracked while moving on a background that by itself elicits a potent OKN and circular vection. The SPS is tested by presenting a visual target on a background. To avoid coactivating the OKS, which is primarily concerned with large-field movement, testing the SPS usually employs small targets moving against featureless backgrounds. Figure 30 shows some of the common pursuit tests.
Tracking Eye Movements to Ramp Stimuli When asked to follow precisely, with their eyes alone, a small target quickly accelerated to a constant velocity from rest—a ramp stimulus (see Fig. 30A)—normal subjects show a great deal of variability. Most often subjects start to move their eyes smoothly after about a 100 to 125 msec latency period but at a velocity less than target velocity.94 The first 100 msec of pursuit is of interest because in this short interval signal processing delays in the visual system are so long that tracking errors do not yet influence the ongoing eye movement and thus reflects the open-loop pursuit response. In some subjects, the magnitude of the initial pursuit response increases with target velocity but for most subjects the magnitude is independent of target velocity.94 To close the increasing target-to-eye disparity after about 200 msec, a saccade ensues that usually leaves the eye short of the target but moving at a velocity greater than target velocity. On close inspection, the velocity profile then shows a few cycles of damped oscillations at about 4 Hz before reaching steady-state tracking with an eye velocity about 0.95 (gain) of the target's velocity to at least 30 degrees/sec.95 For ramp speeds above 30 degrees/sec steady-state pursuit gain decreases, with tracking velocity saturating at about 40 degrees/sec.96 Thus, at 100 degrees/sec ramp velocity SPS gain is about 0.4. With average gains less than 1.0, the eye increasingly lags behind the target's position without the interjection of catch-up saccades. Clearly, the frequency of catch-up saccades increases as SPS gain decreases at high velocities. Occasionally, a few cycles of velocity oscillations similar to those seen at the initiation of smooth pursuit interrupt the steady-state tracking. Catch-up saccades are remarkably accurate, which implies that the brain extrapolates the target's motion while planning the saccade. Indeed, if the target is cleverly stepped in the direction opposite the ramp direction at motion initiation, the first saccade, typically occurring after 200 msec, can often be eliminated (see Fig. 30B). For this to work, the step amplitude is chosen so that the target passes its initial position after a period of time equal to the average saccadic latency (about 200 msec).97 That the saccade does not occur further demonstrates the brain's ability to predict a target's future position and even choose not to make a saccade at all despite the large retinal error initially created by the step. Although the early saccade does not occur, the initial pursuit response is first in the step, rather than ramp, direction demonstrating that the step had not gone unnoticed by the SPS.98 Eye Movements Elicited to Continuously Moving Stimuli Subjects track a sinusoidally moving target (see Fig. 30C) with higher gain than a back-to-back ramp target having the same peak velocity (see Fig. 30D).99 As stimulus frequency increases, SPS gain decreases and more saccades are needed to keep the target image near the fovea.100 Targets moving with a trapezoidal velocity profile (see Fig. 30E) elicit sinusoidal pursuit gains through the central constant-velocity intervals without the harsh turnarounds of the triangle-wave pursuit target. To avoid prediction of target motion, a “physiologically random” target with controllable excursion and peak velocity can be constructed by adding several nonharmonic sinusoids (see Fig. 30F). The role of the fovea in the initiation and maintenance of pursuit has been stressed but extrafoveally cued pursuit is also possible.101,102 Smooth pursuit gain evaluated with sinusoidally moving targets declines with increasing target-to-fovea distance for a given stimulus frequency.102 Vision during Smooth Pursuit Eye Movements Vision during smooth pursuit eye movements is not suppressed, in contrast to the situation with mild suppression during saccadic eye movements. The detection of dim white-light flashes during smooth pursuit eye movement equals detection when the eye is stationary.103 Smooth Pursuit System Plasticity Under certain adapting conditions, SPS plasticity can be demonstrated. Both the initial pursuit response gain106 and the steady state pursuit gain98 are adjustable. Suppression of Vestibulo-Ocular Reflex Suppression (cancellation) of the VOR while watching a target moving with the head is commonly thought to be accomplished by the smooth pursuit system because smooth pursuit and VOR suppression have similar metrics in normals and also because patients with smooth pursuit deficits generally have VOR-suppression deficits. However, clinical reports of patients with smooth pursuit impairment but intact VOR suppression and the converse, VOR-suppression impairment but intact smooth pursuit,105 suggest some independence of pursuit and suppression at some level. VERGENCE SYSTEM Obtaining depth cues through binocular vision depends in large measure on aligning the visual axes of both eyes on the target. Because eyes are spaced apart, the two eyes must rotate disjunctively through different angles as a target moves near and far. The vergence system has evolved to perform this function. As a target moves closer, the eyes (actually the optical axes) converge or diverge as the target moves farther away. The vergence system is but one component of a complex response to targets moving in depth that involves accommodation of the lens to focus the target's image and pupillary changes to improve the depth-of-field; together, these constitute the triadic response. The systems are cross coupled to the extent that disparity, which is nulled by the vergence system, can also drive accommodation, the vergence accommodation response (quantified by the CA/C ratio); similarly, blur, which is nulled by accommodation, can also drive vergence, the accommodative vergence response (quantified by the AC/A ratio); and finally disparity, blur and light level mix to control pupil size. Research has shown that what appears to be voluntary vergence is primarily the cross-coupled convergence of voluntary accommodation.106 In the usual situation in which a new target requires both vergence and saccadic eye movements to be acquired, the two movements may proceed simultaneously, but the result is not a simple sum; the saccade, whether horizontal or vertical, enhances convergence.107 Adaptation in the vergence system has been demonstrated in response to induced phoria by prisms and to changes in effective interocular separation by periscopes (see Miles108 for review of the topic). FIXATION AND MINIATURE EYE MOVEMENTS When a normal subject tries to hold fixation the eye is never absolutely steady. Those small eye movements of less than about 0.5 degrees are referred to as miniature eye movements. Three types are commonly recognized: microdrift, microsaccades, and microtremor.109 Microdrifts are slow. Microsaccades appear to be simply small saccades. In normals, horizontal and vertical microdrift and resetting microsaccades give fixation position an average standard deviation of 0.11 and 0.10 degrees, respectively. Torsional miniature movements show less systematic microdrift with fewer saccades (average standard deviation of 0.18 degrees).110 In some subjects, a small (i.e., less than 2 degrees) saccadic couplet interrupts fixation: the first saccade moves the eye off target, which is refixated by the return saccade approximately 200 msec later. Upward of 20 of these square-wave-jerks per minute may be considered normal.111 |
|
OCULOMOTOR NEUROANATOMY AND NEUROPHYSIOLOGY |
|||||||||||||||
|
Our detailed understanding of ocular motility has resulted because: Eye movements can be precisely measured. Various technologies
have been successfully applied for the measurement of eye movements. Unfortunately,
no single method stands out as being best in all situations. Some techniques
require contacting the eye whereas others do not. DYNAMIC ORBITAL MECHANICS When all torques are acting on the globe balance, the eye is stationary in its orbit. When the torques are not balanced, the eye rotates in the direction of the net unbalanced torque. Active torques are generated by the extraocular muscles driven continuously by brain stem oculomotor motoneurons. Passive torques arise from the various elastic, viscous and inertial elements comprising the orbital contents, however, the inertial torques, arising mainly from the inertia of the globe, are small enough to be ignored.112 In a steady state in which all mechanical elements are at rest, only the elastic components must be resisted by active torque; passive torque generated by viscous elements therefore depends on velocity and thus equals 0. Over the central 90 degrees of horizontal globe movement, the passive orbital elasticity measures about 0.4 g/degree* (line P, Fig. 31, data derived from Collins113). Therefore, to move the eye 10 degrees requires a net torque change of 4 g. Given an intact orbital elasticity (stiffness) of 1.0 to 1.2 g/deg (Fig. 32), the net muscle elasticity (pair) must be about 0.7 g/degree. Interestingly, the stiffness of a single muscle is nonlinear, dropping off as the muscle relaxes (see Fig. 31). The overall linear behavior of the system must come from the opposing arrangement of an agonistantagonist pair having complementary nonlinearities. It is not uncommon in research on the oculomotor system to express torque somewhat inappropriately in gram units. What is implied is that a force, in units equivalent to grams of mass acted on by a 1 G gravitation field, is applied tangentially to the surface of the globe. One routinely calibrates force-measuring devices by hanging on them known measurable weights.
Whenever an unbalanced net torque exists on the globe, the eye moves along a trajectory determined by the interaction of the active and passive torques. The nature of the mechanical elements is such that the output of the system, viewed in the frequency domain, follows inputs of low-frequency sinusoids accurately up to about 1 Hz and increasingly attenuates higher frequency inputs. To generate a saccade, net extraocular muscle torque rises abruptly as the saccade starts, is sustained during the saccade, and decays to a steady, postsaccadic value with an exponential (100 msec time constant) time course (Fig. 33). This waveform is called pulse-slide-step. The pulse and slide reflect combined viscoelastic elements in the orbit; the step holds the eye against elastic restoring forces (see Fig. 31, line P).
OCULOMOTOR MOTOR NUCLEI General Description Three brain-stem nuclei contain neurons that innervate the six extraocular muscles: the abducens nucleus (cranial nerve VI) to the lateral rectus muscle; the trochlear nucleus (cranial nerve IV) to the superior oblique muscle and the oculomotor nucleus (cranial nerve III) to the rest. Abducens Nerve and Nucleus DESCRIPTION. The abducens nucleus is located medially, beneath the floor of the fourth ventricle in the caudal pons (Fig. 34). The nucleus proper contains motoneurons intermingled with internuclear neurons. Segregated along the dorsal aspect of the abducens nucleus are neurons that project to the cerebellar flocculus114 and are best included with other neuronal groups of the “paramedian tracts.”115
OUTPUTS. Two output paths: VI cranial nerve to innervate ipsilateral lateral rectus muscle and medial longitudinal fasciculus (MLF) to innervate reticular formation (RF) and the nucleus of the sixth cranial nerve, which exits the brain stem ventrally, along the medial pontomedullary junction. It then courses forward and laterally, crossing over the petrous bone and traversing the cavernous sinus to enter the orbit through the superior orbital fissure and innervate the lateral rectus. Axons of internuclear neurons cross the midline at the level of the abducens nucleus before joining the MLF and project to the medial rectus subdivision of the oculomotor nucleus (Fig. 35). Some abducens internuclear neurons send axon collaterals into the neighboring brain stem.116,117
INPUTS. The abducens nucleus receives input principally from the oculomotor nucleus (oculomotor internuclear neurons), the pontine and medullary RF (excitatory and inhibitory burst neurons), the vestibular nuclei, and from the perihypoglossal complex.118 NEURAL RECORDINGS. For all types of eye movements, initiation of globe rotation lags behind the neural control recorded in the brain stem by about 5 to 8 msec. This delay reflects spike conduction time along the nerve, neuromuscular junction delay, and muscle activation delays. Over a period of a few seconds during fixation, the motoneuron firing rate is remarkably constant with variability (standard deviation) about 6% of the mean (Fig. 36A).36 The steady-state, postsaccadic firing rate after saccades all ending in the same position fluctuates. Some observed variability depends on direction (hysteresis) and some reflects slowly modulating cocontractive noise.119 While looking in the direction of the innervated muscle's action, the ON direction, the motoneuron firing rate increases monotonically and is linearly related to eye position for much of the oculomotor range (Fig. 36B). Conversely, as the animal looks in the opposite direction, the OFF direction, motoneuron activity decreases. At some orbital position, the neuron's threshold position, ET, activity ceases entirely. When the eye is positioned within a few degrees to the ON side of ET, activity is erratic so that ET is estimated by plotting firing rate against eye position (rate-position curve) and extrapolating to meet a 0 firing rate. The mean value of ET is 25 degrees in the OFF direction (0 degrees is primary position, straight ahead) and ranges from 25 degrees in the ON direction to 62 degrees in the OFF direction. At primary position, about 50% of the motoneuron population is active (see Fig. 27) with an average of 100 spikes/sec firing rate. The slope of the rate-position curve, k, averages about 3.5 (spikes/sec)/deg and ranges between 1.1 and 14.5 (spikes/sec)/deg.36,120,121 Some evidence indicates that for some motoneurons increased convergence alters the rate-position curves by shifting them upward to somewhat less steep slopes.122 In summary, for steady fixation and convergence state, the motoneuron behavior can be stated
(1) RMN = k(E - ET) where RMN is motoneuron firing rate, E is eye position, and k and ET are constants. A histogram of ET depicts the recruitment ordering for the oculomotor system (see Fig. 24). Of note also is a moderately strong relation between ET and k: k values tend to be lower as ET is further in the OFF direction.119 Equation 1, however, needs to be modified to hold when the eye moves at a constant velocity. An additional term depending on eye velocity, E®, must be added. (2) RMN = k(E - ET) + rE® (see Fig. 36C and D). The value for r averages 0.95 (spikes/sec)/(degree/sec) with a range from 0.25 to 5.0 (spikes/sec)/(degree/sec).120 Equation 2 has been shown to describe motoneuron activity for smooth pursuit and low-frequency vestibularly induced slow eye movements adequately.123 The ratio r Þe0 k represents the dominant low frequency low-pass time constant of the oculomotor plant and averages about 200 msec. During saccadic eye movements in which the eye moves transiently, the firing rate behavior defies description as a differential equation such as Equation 2. Qualitatively, Figure 37 depicts the phases of activity (ignoring delays). Phase 1 is the constant presaccadic activity associated with the rate-position relation (see Eq. 1). When the neuron is driving the agonist muscle the firing rate jumps quickly (Phase 2) to a high level (Phase 3, usually about 600 to 700 spikes/sec in monkeys). The temporal variability of this transition in any one neuron for repeated identical saccades is usually within 1 msec (unpublished observation). There is never a preamble during Phase 1 that anticipates the upcoming saccade. The high per-saccadic activity (Phase 3), called the saccadic burst, is usually jagged and is rarely uniform even after averaging (unpublished observation). During large saccades (i.e., 20 degrees) the firing rate tends to diminish somewhat during the burst but is sustained for more than 90% of the saccadic duration. In comparison, during small saccades (i.e., 5 degrees) the per-saccadic burst is hardly sustained, the high frequency burst lasts only a small fraction of the saccade duration.124 In addition, for small saccades, the peak burst rate increases as the small saccades are tested further in the ON direction. Large saccades fail to show such position dependence.121
At the end of the saccade, the neuron's activity is not yet at a steady level. Instead the rate decays for approximately the next 500 msec in two phases. In monkeys, Phase 5 can be approximated by an exponential having a mean amplitude of 45 spikes/sec and time constant of 0.072 sec. This has led to the pulse-slide-step description of saccadic generation.124,125 Phase 6 has never been measured systematically but accounts for only a small component of the neural control. When the motoneuron drives the antagonist muscle during a saccade, the firing rate drops quickly before the saccade begins. For sufficiently large saccades, the neuron is completely inhibited. Often a neuron is silent early in the saccade but becomes active during the saccade. After the saccade, the rate continues to rise exponentially with a time constant of 0.090 sec (see Fig. 37, phase 5, lower trace), mirroring the postsaccadic exponential decay in rate after oppositely directed saccades.124 Therefore, this waveform is described as pause-slide-step. LESIONS. Because abducens interneurons carry the horizontal conjugate signal destined for the medial rectus it is impossible to cause a totally isolated sign from the sixth cranial nerve from a sixth cranial nerve nuclear lesion. Instead, the cause of isolated paralysis of the sixth cranial nerve is usually in the pons away from the sixth cranial nerve nucleus (e.g., pontine glioma), or outside the pons where the nerve is subject to microvascular infarction, to pressure from basilar artery branches with generalized increase in intracranial pressure, to pressure from tumors, and to inflammations such as meningitis, middle ear infection (Gradenigo's syndrome), or with infections of the cavernous sinus or orbit. Such lesions upset the generation of torque so that some eye positions become unreachable and saccades become hypometric, with excessive postsaccadic drift. Oculomotor Nerve and Nucleus DESCRIPTION. The nucleus is located in the midbrain along the ventromedial aspect of the periaqueductal gray (see Fig. 34). The motoneuron cell bodies for each muscle cluster together within the oculomotor nucleus forming nuclear subdivisions innervating a single muscle (Fig. 38). Among the motoneurons in the medial rectus subdivision are found internuclear neurons projecting to the abducens nuclei, mostly contralaterally.118 Cells within the Edinger-Westphal nucleus and the anteromedian nuclei, classically related to pupil and accommodation, give an appearance of regular motor neurons but complete iridectomy alone affects only a small fraction (about 3%) of these cells.126 Westheimer and Blair found that paralysis of synaptic transmission in the ciliary ganglion affected accommodation to a minimal degree, and probably some of these cells directly control accommodation via the ciliary muscles without an intervening ciliary ganglion synapse.127
OUTPUTS. Motoneuron axons leaving the superior rectus and (in part) the levator palpebrae subdivisions cross the midline at the level of their cell bodies and exit with the contralateral oculomotor nerve.128 Motoneuron axons leaving the remaining subdivisions enter the ipsilateral oculomotor nerve. Each oculomotor nerve contains about 24,000 nerve fibers and sources the innervation for the superior rectus, inferior rectus, medial rectus, inferior oblique, and levator muscles of the upper lid, as well as the parasympathetic innervation to the intraocular muscles. After leaving the brainstem, the third cranial nerve courses anteriorly, passing near the anterior-posterior cerebellar artery and the posterior cerebral artery, before piercing the dura on its way forward. In this area, the nerve remains especially vulnerable to pressure from an aneurysm and from herniation of the uncus through the tentorium with increased supratentorial pressure. The third cranial nerve divides into a superior branch to the levator and superior rectus muscles and an inferior branch carrying the innervation to the intraocular muscles and to the inferior rectus, medial rectus, and inferior oblique muscles. This separation can become distinct even as the nerve enters the cavernous sinus, and lesions of either branch alone can occur. INPUTS. These include the interstitial nucleus of Cajal (NIC), the rostral interstitial nucleus of the medial longitudinal fasciculus, the pretectum, the abducens nucleus (abducens internuclear neurons), the vestibular nuclei, the perihypoglossal complex.129 LESIONS. Because of the contralaterally projecting superior rectus and levator cell groups, a lesion of the third cranial nerve nucleus does not cause a unilateral paralysis, and a third cranial nerve palsy involving the levator and superior rectus, as well as other muscles supplied by that nerve, is almost certainly caused by a nerve lesion. When the nerve has been injured, regrowth of the nerve fibers ensues, sometimes into the wrong perineurial channels (aberrant regeneration). In such cases, some combinations are especially common; for example, a fiber to the inferior rectus may find its way into the levator muscle, causing elevation of the lid on downward gaze (pseudo-Graefe sign). Trochlear Nerve and Nucleus Description. The trochlear (sixth cranial) nerve arises from a small nucleus lying immediately dorsal to and indenting the medial longitudinal fasciculus at the level of the rostral portion of the inferior colliculus (see Fig. 34). INPUTS. These arise in the contralateral medial vestibular nucleus and ventrolateral vestibular nucleus by means of axons ascending in ipsilateral MLF130; interstial nucleus of Cajal131; and ipsilateral riMLF.132 OUTPUTS. The fourth cranial nerve, which is the only ranial nerve that exits the brain stem from its dorsal aspect, courses dorsally into the superior medullary velum before crossing to the opposite side. Having been freed from the velum caudal to the inferior colliculus, the nerve runs a long and exposed course ventrally and forward to the cavernous sinus, and then through the superior orbital fissure, to innervate the superior oblique muscle. NEURAL RECORDINGS. Activity decreased during convergence in all cells tested to a degree greater than with conjugate adduction.133 LESIONS. The trochlear nerve is, not surprisingly, peculiarly susceptible to rather minor head trauma, possible because of stretching or compressing during its tortuous passage. Neuropathology of head-injury victims has also shown tears of the nerve rootlets emerging from the brain stem and tears of the superior medullary velum, providing additional mechanisms for palsy in some cases. Spontaneous onset of fourth cranial nerve weakness and subsequent recovery is not rare and may arise from occlusion of small vessels.134 VESTIBULAR SYSTEM Vestibular Nerve NEURAL RECORDINGS. Afferent fibers recorded in the vestibular division of the vestibulocochlear (cranial nerve VIII) relay information arising from either rotational forces or translational forces acting to move the head. Those carrying rotational information innervate hair cells in one of the three ipsilateral semicircular canals, whereas those carrying translational-force information innervate one of the two otolith organs, the saccule or utricle (Fig. 39A). Because gravity is a translational force, the otolith organs sense head tilt, as well. In each labyrinth, the three semicircular canals (anterior, posterior, and horizontal) are oriented in approximately perpendicular planes. The two labyrinths are positioned in the skull such that the right and left horizontal canals lie in approximately parallel planes, as do the anterior canal on one side and the posterior canal on the other (see Fig. 39B). Because canals in parallel planesdetect head rotation around the same axis, only three independent rotational signals are measured, but because of mirror-image symmetry, when one canal of a parallel pair is excited, the other is inhibited.
Most primary vestibular neurons have a significant resting discharge rate in the absence of vestibular stimulation; however, some have a more regular discharge rate than others. Stimulation of the labyrinth causes a modulation of the afferent discharge rate. An average canal afferent responds to the onset of constant head velocity with an initial step change proportional to the velocity, but because force is not sustained (constant velocity) the activity decays back to the resting rate following an exponential time course having a 5.7 second time constant in primates (Fig. 40).135 This decay is thought to reflect the time course of cupular relaxation and is taken as the cupular time constant. Therefore, after about 17 to 18 seconds following a change to a steady velocity, the neural signal arising from the vestibular periphery has returned to the resting discharge rate and thus fails to carry any information about the ongoing head movement. The value of the cupular time constant is about one third of the VOR time constant.
Vestibular Nuclei DESCRIPTION. Six brain nuclei receive direct input from the vestibular nerve. Four comprise the classical vestibular nuclei: medial, superior, inferior, and lateral (Fig. 41). The py-group and basal interstitial nucleus complete the set. Primary vestibular input also reaches the cerebellar vermis.
INPUTS. After bifurcating (the usual situation) on entry into the medulla, primary vestibular input distributes nonuniformly to regions of each nucleus. Additional input is through the cerebellum (flocculonodular lobe136 and uvula), the contralateral vestibular nuclei,137 intrinsic connections between nuclei, nucleus preposititus,138 NIC, and posterior parietal cortex.139 OUTPUTS. To ocular motor nuclei, these neurons are mostly confined to the rostral medial vestibular nucleus, the superior vestibular nucleus, the ventrolateral vestibular nucleus, and the y-group. Other output targets include the nucleus prepositus138 and flocculus.114 Cells related to the horizontal VOR are found in the medial and ventral lateral vestibular nuclei and form three major types based on output morphology.140 One type projects exclusively to contralateral targets, which include the abducens nucleus, nucleus prepositus, RF, and vestibular nuclei. Another type has ascending ipsilateral projections primarily to the medial rectus subdivision of the oculomotor nucleus. The final type projects ipsilaterally, predominantly to the abducens and prepositus nuclei. Cells related to the vertical VOR are found in the medial, ventral lateral, and superior vestibular nuclei and form two major types based on output morphology.130 The axon of one type ascends within the ipsilateral MLF to terminate in the ipsilateral trochlear and oculomotor nuclei; the axon of the other type ascends within the contralateral MLF to terminate in the same contralateral nuclei. Other cells in the vestibular nuclei give rise to mossy fibers innervating the cortex of the cerebellar flocculus and posterior vermis,141,142 and a projection to the nearby nucleus prepositus.138 NEURAL RECORDINGS. Recordings from neurons in the vestibular nuclei reveal an abundance of eye movement-related activity, in addition to vestibular activity.143 Many cells are excited by horizontal vestibular rotation in one direction and optokinetic stimulation in the other: the increased activity continues during optokinetic after-nystagmus suggesting that these cells are in the indirect optokinetic pathway.144 The most prevalent type of vestibular cell projecting to the vertical oculomotor motor nuclei through the MLF, called tonic-vestibular-pause (TVP) cells (also called position-vestibular-pause or PVP cells), carries a nonsaccadic eye movement signal, pauses for all saccades except perhaps saccades in the ON direction with respect to the eye movement sensitivity, and modulates their activity in response to head velocity145 (see Fig. 41). NUCLEUS PREPOSITUS DESCRIPTION. A dorsomedial column of cells that ranges from the rostral pole of the hypoglossal nucleus (cranial nerve XII) in the upper medulla to the caudal pole of the abducens nucleus in the lower pons and is one of the perihypoglossal nuclei (see Fig. 41). INPUTS. Included are the vestibular complex, pontine RF (likely including saccadic excitatory burst neurons [EBNs]), the perihypoglossal nuclei, the extraocular motor nuclei (except the trochlear nucleus), and the deep cerebellar nuclei (fastigial nucleus).138 OUTPUTS. These include the vestibular and perihypoglossal nuclei, the inferior olive, the medullary RF, the extraocular motor nuclei and parts of the cerebellum (including the vestibulocerebellum).138 INFERIOR OLIVE DESCRIPTION. The inferior olive forms a conspicuous nuclear complex in the ventrorostral medulla and sources climbing fibers that terminate on Purkinje cells of the cerebellar cortex, with collaterals directed to the deep cerebellar nuclei. So far, only two subgroups of the medial accessory olivary (MAO) division have been linked to eye movement control: the dorsal cap of Kooy and subnucleus b. The olivocerebellar system has been shown to be an important substrate mediating plasticity of the VOR.146 INPUTS. The dorsal cap obtains input from the pretectal nuclei,147 the accessory optic system nuclei,147 and nucleus prepositus.138 Subnucleus b obtains input from the superior colliculus148 and nucleus prepositus.138 Additional weak input comes from the NIC.131 OUTPUTS. These include the dorsal cap to the flocculus, subnucleus b to vermis lobule VII149 and to the fastigial nucleus.150 NEURAL RECORDINGS. For this topic, see discussion under Cerebellum, climbing fiber input. BRAIN-STEM RETICULAR FORMATION GENERAL DESCRIPTION. Portions of the RF extending from the rostral medulla to the rostral midbrain contain neurons that participate in eye movements (see Fig. 34). Three regions are important: the paramedian pontine (or pontomedullar) reticular formation (PPRF), the nucleus reticularis tegmenti pontis (NRTP), and the mesencephalic reticular formation (MRF). Paramedian Pontine Reticular Formation DESCRIPTION. Three nuclei are involved with an oculomotor function: nucleus reticularis pontis caudalis, nucleus paragigantocellularis pars dorsalis, and nucleus raphe interpositus. NEURAL RECORDINGS. Nucleus reticularis pontis caudalis and nucleus paragigantocellularis pars dorsalis contain horizontal burst neurons, so-called because they burst maximally for ipsilateral horizontal saccades, burst less vigorously for vertical saccades, burst weakly or not at all for contralateral saccades, and are silent between saccades.151,152 By contrast, omnipause neurons (OPNs) in nucleus raphe interpositus maintain a high tonic spike rate that ceases completely during saccades153 about 16 msec before the saccade begins.154 INPUTS AND OUTPUTS. Burst neurons in nucleus reticularis pontis caudalis project directly and heavily to and excite neurons in the ipsilateral abducens nucleus (see Fig. 35) and are thus referred to as horizontal EBNs.151,155 Burst neurons present within the nucleus paragigantocellularis pars dorsalis are inhibitory and thus called inhibitory burst neurons (IBNs). Unlike EBNs, IBNs project almost exclusively to contralateral areas, especially the contralateral abducens nucleus.152 Additionally, EBN collaterals project to the ipsilateral IBN area, nucleus prepositus, and the medial vestibular nucleus with a minor projection to other pontine reticular areas rostral to the abducens nucleus. Other contralateral targets include all vestibular nuclei, the EBN area, and nucleus prepositus. OPNs terminate on EBNs and IBNs.156 Input to the OPNs is from PPRF, and more modestly from nucleus of Cajal and the adjacent mesencephalic RF, the superior colliculus, the region dorsolateral to the NRTP, and the medial vestibular nucleus.157 MICROSTIMULATION. Electrical stimulation of the OPN region causes complete elimination of both horizontal and vertical saccades: vestibular and optokinetic slow eye movement continue.158 LESIONS. Unilateral chemical lesions of the caudal PPRF knock out saccades and quick phases toward the side of the lesion.159 Lacking nystagmus during horizontal vestibular stimulation toward the lesioned side, the eyes deviate fully in the orbit away from the lesion. Bilateral lesions at this same level abolish all saccades in all directions. In response to either vestibular or optokinetic stimulation, the eyes slowly deviate in the orbit appropriately showing that eye movement, in itself, was not limited by the lesion. Finally, bilateral lesions of the rostral PPRF abolish horizontal saccades and quick phases without affecting vertical saccades and quick phases. Nucleus Reticularis Tegmenti Pontis DESCRIPTION. A massive nucleus found dorsal to the basis pontis. INPUTS. These include the medial visual association cortex,160 the frontal eye field (FEF),161 the supplementary eye field (SEF),162 the inferior parietal lobule (weak),163 the ipsilateral nucleus of the optic tract (NOT),164 the superior colliculus,148 and the contralateral fastigial nucleus.165 OUTPUTS. The dorsomedial NRTP projects to posterior vermis,166 flocculus,114 and ventral paraflocculus167; a lateral cell group provides a source for additional floccular input.114 NEURAL RECORDINGS. Most cells in the dorsomedial NRTP discharge a burst of spikes before and during saccadic eye movements into the cell's retinotopically organized movement field regardless of whether the saccade was visually triggered or spontaneous.168 A separate small group of NRTP neurons becomes tonically active when attending a visual target either during fixation of a stationary target or during smooth pursuit and pauses irregularly for saccades169; some cells in medial NRTP have activity related to the near-or-far response.170 MICROSTIMULATION. Mostly smooth upward eye movements result from stimulating sites associated with pursuit activity in rostral NRTP171; microstimulation at sites where near or far response neurons were recorded often produced changes in vergence angle and accommodation.170 Mesencephalic Reticular Formation INPUTS. These arise in the deep layers of the superior colliculus,172 NOT,164 ipsilateral NIC,131 SEF,162 and ispilateral FEF to lateral MRF.161 OUTPUTS. Targets include the nucleus prepositus,138 central MRF to flocculus,167 fastigial nucleus,172 SEF,162 visual cortical areas 17 and 18,173 and MRF adjacent to the NIC to nucleus raphe interpositus (OPNs).157 NEURAL RECORDINGS. Central MRF (nucleus subcuneiformis) contains cells that show a burst of activity in relation to all horizontal saccades.174 In an area just dorsal to the oculomotor nucleus, neurons can be found that change their discharge rate for vergence.175 Some neurons show increased activity during convergence, others for divergence. MICROSTIMULATION. Contralateral saccades of site-dependent amplitude are elicited when central MRF is stimulated unilaterally. Saccades are suppressed on bilateral stimulation.176 CEREBELLUM GENERAL DESCRIPTION The cerebellum is variably involved in the processing of oculomotor signals but eye movements are still possible even after total cerebellar ablation.177,178 Consistent findings following cerebellar lesions include: (1) impairment of smooth pursuit function, (2) impairment of VOR suppression by small visual targets, (3) loss of the rapid rise in optokinetic slow phase velocity, (4) saccadic dysmetria, and (5) gaze-evoked nystagmus. More closely refined experiments have defined specific cerebellar areas concerned with eye movements. Flocculonodular Lobe/Ventral Paraflocculus DESCRIPTION. The flocculus is the hemispheric portion of the flocculonodular lobe, the caudalmost and phylogentically oldest cerebellar area. Cerebellar folding is such that the flocculus lies with the eighth cranial nerve in the cerebellopontine angle. INPUTS. Similar to cerebellar cortex generally, input to the flocculus is through two routes: climbing fibers and mossy fibers. Climbing fibers arise from cells in the contralateral inferior olive (dorsal cap of Kooy of the medial accessory subdivision).114 Mossy fibers arise from vestibular and pontine nuclei and from the NRTP. Using neuroanatomic tracers, primary vestibular input to the flocculus from the vestibular nerve, often mentioned in neuroanatomy texts, has been denied in research monkeys. Floccular Purkinje cells project exclusively to the oculomotor portions of the ipsilateral vestibular nuclei and a published study described basal interstitial nucleus of the cerebellum.136 Flocculus: ipsilateral vestibular ganglion, bilaterally from the vestibular and prepositus hypoglossal nuclei, NRTP, the central mesencephalic RF. VP receives mossy afferents mainly from the NRTP and pontine nuclei and sparsely from the vestibular system.167 OUTPUTS. Within the flocculus, these include medial and ventrolateral parts of the medial vestibular nucleus, superior vestibular nucleus, and y-group. For the ventral paraflocculus: caudal ventral part of posterior interpositus and dentate nuclei and medial and ventrolateral parts of the medial vestibular nucleus, as well as the superior vestibular nucleus and y-group.167 NEURAL RECORDINGS. Neural recordings from the flocculus reveal that the activity of 93% of Purkinje cells modulate during eye movement, many during smooth pursuit.179 Floccular Purkinje cells show increased simple spike activity during the initial rise in OKN slow phase velocity with a return to resting levels during optokinetic after-nystagmus suggesting that floccular Purkinje cells are part of the direct optokinetic pathway and not concerned with velocity storage.180 Input from the contralateral inferior olive, as measured by complex spikes, transmits the retinal slip velocity resulting from pursuit errors. Complex-spike rate is inversely rated to simple spike rate during pursuit.181 Activity during vestibular and OKN stimulation betray two different mossy fiber inputs: One class saturated at a velocity of 60 degrees/sec during optokinetic stimulation (as is found in the vestibular nuclei) while another carried retinal image slip information. Purkinje cells were modulated in their simple spike activity during optokinetic stimulation only at stimulus velocities above 40 to 60 degrees/sec.182 MICROSTIMULATION. Nodulus: long duration, low current pulse trains evoke vigorous nystagmus having a contralateral slow phase with a prolonged, similarly directed afternystagmus183; time constant of horizontal postrotatory nystagmus and OKAN are reduced.184 LESIONS. Flocculus and/or ventral paraflocculus: vision-induced postsaccadic drift adaptation is abolished185; direct optokinetic path attenuated186; OKAN (and thus velocity storage) continue after lesions,186 as do phoria adaptation to prisms and AC/A adaptation to periscopes187; Nodulus: failure of vision to reduce time constant of OKAN.188 Surgical inactivation of the cerebellar nodulus and ventral uvula abolishes the steady-state nystagmus during constant velocity, off-axis rotation.189 Posterior Vermis DESCRIPTION. Cerebellar lobules VIc and VII comprise the oculomotor vermis. INPUTS. Mossy fiber input to lobule VII comes primarily from the medial and dorsolateral portions of the NRTP and the pontine nuclei.166 Climbing fiber input arises exclusively from the medial accessory division of the inferior olive (subnucleus b). OUTPUTS. These are found within the fastigial nucleus.172 NEURAL RECORDINGS. Purkinje cell simple-spike discharge is related to saccadic,190 smooth pursuit, and vestibular eye movements.191 MICROSTIMULATION. Low current (less than 10 μA) stimulation evokes conjugate, generally oblique (but with ipsilateral horizontal components) saccades even when the animal actively attends a small visual target.191 LESIONS. Lesions induce lasting hypermetric saccades without postsaccadic drift.192 Deep Cerebellar Nuclei DESCRIPTION. The deep cerebellar nuclei form a conspicuous group within the cerebellar medullary white matter. By way of anatomic tracing and neural recording, a part of the fastigial nucleus, the fastigial oculomotor region (FOR), has been identified. INPUTS. FOR receives bilaterally from Purkinje cells in ipsilateral oculomotor vermis, subnucleus b of the contralateral medial accessory olive, NRTP, vestibular nuclei, and reticular nuclei.172 OUTPUTS. Most FOR output fibers decussate within the cerebellum and enter the brain stem through the contralateral uncinate fasciculus.172 Those fibers related to horizontal saccadic components enter the descending limb of the fasciculus and project bilaterally to nucleus prepositus and138 NRTP.166 Fewer fibers carry the vertical component to the midbrain (rostral interstial nucleus of the MLF and mesencephalic RF) through the contralateral superior cerebellar peduncle.193 NEURAL RECORDINGS. Saccade-related activity can be recorded from each deep cerebellar nucleus but the timing of the signals is usually too near the onset of the saccade to have caused it.194 Cells in the rostral fastigial nucleus increase firing during contralateral head rotations and ipsilateral optokinetic stimuli but are unmodulated during saccades or pursuit. Neurons in the caudal fastigial nucleus respond during vestibular and pursuit195 eye movements. MICROSTIMULATION. The dorsal fastigial nucleus (i.e., FOR) is a low-threshold region for eliciting saccades.196 PONTINE NUCLEI Dorsolateral Pontine Nucleus INPUTS. These are widespread from cortical areas including the FEFs,161 parieto-temporo-occipital cortex,197 posterior parietal cortex,198 and NOT. OUTPUTS. These occur within the cerebellar flocculus114 and vermis.199,200 NEURAL RECORDINGS. Neurons respond variably to movement of visual targets and smooth pursuit eye movements.201,202 Almost all neurons related to smooth pursuit activity responded most strongly to movement in a particular direction. Activity of cells driven by visual stimuli increased before pursuit was initiated whereas activity of cells driven by smooth pursuit only increased as or after pursuit was initiated. LESIONS. Findings include major pursuit and OKN (direct pathway) deficits after chemical lesions.203 SUPERIOR COLLICULUS DESCRIPTION. These paired tectal nuclei histologically appear faintly laminated, with mostly cellular layers between mostly fiber layers. INPUTS. Superficial layers: topographic input from the retina through the brachium of the superior colliculus and from visual cortical areas (including 17, 18, and 19),204 FEF,204 and the temporo-occipital association cortex in topographic register with striate input.205 Deep layers: frontal cortex (including the FEF)206; posterior parietal cortex207; substantia nigra, the midbrain tegmentum, the NRTP, and the medial RF208,209; and the NOT.164 OUTPUTS. Superficial layers: pretectum, including the NOT, the parabigeminal nucleus, and the pulvinar and lateral geniculate nucleus.210 Collaterals terminate in the deep layers immediately below.211 Deep subcutaneous layers: regions of the thalamus connected to the FEF and area 7 of the parietal lobe, the midbrain and pontine RF (especially the NRTP), and the medial accessory inferior olive.148,210 NEURAL RECORDINGS. Superficial layers: most neurons activated by visual targets within the cell's receptive field where most of these cells respond transiently to the presentation of a stationary spot with activity at stimulus onset and offset and respond to movement of the spot through the receptive field in any direction.212 Other visual cells are directionally selective. Intermediate layers: activity of many cells in the deep subcutaneous layers precede saccadic eye movements within the cell's movement field,213 many discharging equally well for the appropriate visually guided or spontaneous saccades, or the quick phase of vestibular nystagmus.214 Movement fields are predominantly situated in the contralateral visual field and are generally in the same area as the receptive fields in those cells that can, in addition, be driven by visual stimuli. During short-term saccadic adaptation, activity of saccade-related neurons in the subcutanous layer code the saccade required to foveate the initial target, rather than the adapted saccade.215 MICROSTIMULATION. Electrical stimulation of the subcutaneous with a short pulse train elicits only conjugate, saccadic eye movement with contralateral horizontal components. The specific size and direction are almost independent of initial eye position or stimulus current but do depend on the particular site stimulated: large (small) saccades are elicited caudally (rostrally) and saccades with up (down) vertical components are elicited at medial (lateral) collicular positions.216 Continuous stimulation produces a series of nearly identical saccades spaced about 100 msec apart. At a particular site, the elicited saccade usually moves the eye into the associated visual receptive field.217 LESIONS. Bilateral ablations do not eliminate saccades; however, lesions do have effects, some enduring, some not. Just after unilateral subcutaneous ablation, monkeys make few saccades to targets in the contralateral peripheral visual field.218 The defect appears to be sensory 219 and recovers in 2 to 4 weeks.218 Saccadic latency increases by 100 to 200 msec initially and recovers somewhat but not to prelesion values.220 The short-latency express saccades never recover.81 These observations, combined with the finding that paired collicular and FEF lesions have a devastating and lasting effect on saccadic range, frequency, and velocity, whereas lesions of each area alone produce primarily transient deficits, suggest that saccade generation can be effected through two pathways, one involving the superior colliculus and the other the FEFs.218 INTERSTITIAL NUCLEUS OF CAJAL DESCRIPTION. One of the midbrain accessory oculomotor nuclei, the NIC contains cells of multiple shapes. OUTPUTS. Three output systems: posterior commissural system to contralateral NIC, oculomotor and trochlear nuclei; descending system to ipsilateral RF and spinal cord heavily, vestibular nuclei and nucleus prepositus moderately; ascending system to ipsilateral mesencephalic RF and zona incerta, and to riMLF. NUCLEUS OF THE OPTIC TRACT AND THE DORSAL TERMINAL NUCLEUS DESCRIPTION. Both the NOT, classically included in the group of pretectal nuclei, and the dorsal terminal nucleus (DTN) of the accessory optic tract, classically included as one of the accessory optic system nuclei, are situated in the midbrain along the ventral edge of the brachium of the superior colliculus, the NOT positioned immediately dorsomedial to the DTN.221 INPUTS. NUCLEUS OF THE OPTIC TRACT. These are direct, mostly contralateral but also bilateral, retinal projection through the brachium of the superior colliculus,222 and superficial layers of the superior colliculus.210 DORSAL TERMINAL NUCLEUS. Retinal projection occurs through the accessory optic tract.221 OUTPUTS-NUCLEUS OF THE OPTIC TRACT. Ipsilateral DTN and contralateral NOT/DTN. NUCLEUS OF THE OPTIC TRACT/DORSAL TERMINAL NUCLEUS. Inferior olive, contralateral oculomotor complex, dorsolateral and dorsomedial pontine nuclei, and NRTP are found, but also weakly to the ipsilateral nucleus prepositus.138,147,164 MICROSTIMULATION. This process evokes horizontal nystagmus with slow phases toward the side stimulated.219 Nystagmus lacks rapid rise in slow phase velocity with stimulation onset and after-nystagmus continues with stimulus offset suggesting that the NOT and DTN are part of the indirect optokinetic pathway that feeds into the velocity storage element. NEURAL RECORDINGS. The neurons in the NOT/DTN projecting to the inferior olive are excited when large- or small-area visual targets, presented to either eye, move ipsiversively and are inhibited by motion oppositely directed.147 LESIONS. Unilateral NOT lesions abolish ipsilaterally directed OKN but spare saccadic and smooth pursuit eye movement.222 ROSTRAL INTERSTITIAL NUCLEUS OF THE MEDIAL LONGITUDINAL FASCICULUS DESCRIPTION. A cytologically separate neuronal group in the rostral mesencephalic RF lying ventral to the nucleus of Darkschewitsch and rostral to the NIC and the tractus retroflexus.224 INPUTS. These come from the caudal PPRF (presumably omnipause cells) and vestibular nuclei.224 OUTPUTS. These include the ipsilateral oculomotor and trochlear nuclei.132,225 NEURAL RECORDINGS. Cells have responses similar to burst neurons in PPRF, but with upward or downward ON directions.132,225 LESIONS. Unilateral lesions abolish torsional rapid eye movements in which the ipsilateral eye extorts and contralateral eye intorts but do not abolish vertical saccades. Bilateral lesions abolish vertical and torsional saccades permanently.226 THALAMUS DESCRIPTION. Based on histology and connections, the thalamus is partitioned into numerous subnuclei. Only a few of these have known oculomotor activity. NEURAL RECORDINGS. Intralaminar nuclei: activity herein is associated with saccades, smooth pursuit eye movement, and fixation, as well as with the presentation of visual targets227; Pregeniculate nucleus: cells discharge after the onset of saccades in the dark223; ventral posterolateral nucleus (VPLO): vestibular function represented in a small number of cells distributed throughout the oral part.228 INPUTS AND OUTPUTS. VPLO receives a direct bilateral projection from the vestibular nuclei229; weak to moderate bilateral labeling of the dorsomedial, central medial, and central lateral nuclei after orthograde tracer injection into the NIC131; input from occipitotemporal association cortex (areas MST and FST) to reticular nucleus230; ventral anterior (VA) and dorsomedial (DM) have reciprocal connections with the supplementary and FEFs (SEF and FEF)231; and input from fastigial nucleus.172 MICROSTIMULATION. The saccade target is modified when the central thalamus is microstimulated.232 HUMAN FUNCTIONAL IMAGING. Right posterior thalamus activation occurs during execution of visually guided saccades (PET study).233 BASAL GANGLIA DESCRIPTION. Modern discussions consider the putamen and caudate nucleus (together called the striatum), globus pallidus, subthalamic nucleus, and substanitia nigra components of the basal ganglia. INPUTS. Parts of the FEFs from which saccades can be evoked electrically project topographically to the striatum through fibers passing near the genu of the internal capsule and to the claustrum through the external capsule.234 A FEF projection to the subthalamus does not appear to be topographic.229 OUTPUTS. The striatum, in turn, projects to the substantia nigra pars reticulata, which projects to the superior colliculus. NEURAL RECORDINGS. Nigral neurons related to eye movement respond variably to visual and motor events. These cells, which, when unstimulated, have a high background discharge rate, respond to stimulation with a decrease in discharge rate. The activity of many nigral neurons is modulated before saccades to visual targets but do not respond to spontaneous saccades made randomly in the dark.235 Some cells respond when a saccade is made to a previously lit and thus remembered target.235 Many of the saccade-related nigral cells can be antidromically activated from the superior colliculus suggesting that these nigral cells project to the superior colliculus. Further investigations have identified γ-aminobutyric acid as the neurotransmitter likely used in the nigrocollicular pathway, where it produces an inhibitory effect on the collicular target cells.236,237 Before a saccade, this inhibition is removed, freeing the collicular cells to initiate the saccade. CEREBRAL CORTEX GENERAL DESCRIPTION. There is no single cortical oculomotor center. Instead, eye movement processing is distributed across various association areas. This section summarizes the findings about those oculomotor cortical regions that have been probed extensively (Fig. 42).
Occipital Cortex LESIONS. Immediately following bilateral extirpation of striate cortex in monkeys, small visual stimuli failed to elicit eye movements; spontaneous saccades and full-field OKN (but without the normal initial jump in slow-phase velocity) could still be made, however.238 After several months of recovery, a surprising amount of visually guided eye movement was regained. Accurate saccades could be made to smaller visual targets but with somewhat longer latencies than normal. Tracking of a small moving target, which immediately after surgery was saccadic, later was accomplished by the smooth pursuit system but with longer than normal latencies to initiate pursuit. Clearly extrastriate visual pathways are capable of generating goal-directed eye movement. Cortex at Temporal and Occipital Lobe Junction DESCRIPTION. The two subregions MT and MST in the monkey's dorsal superior temporal sulcus have been shown to process visual motion. A human homologue has been located along the ascending limb of the inferior temporal sulcus (see Fig. 42).239 INPUTS AND OUTPUTS. Area MT receives a retinotopic, ipsilateral projection from visual cortex through arcuate fibers.197 In turn, area MT projects to MST through the arcuate fibers, the lateral pontine nuclei through a pathway including the internal sagittal stratum, and the contralateral MT and MST areas through the tapetum and corpus collosum. Area MST projects to posterior parietal cortex through arcuate fibers, the accessory optic system, and lateral pontine nuclei through the internal capsule and the contralateral MST area through the corpus collosum. LESIONS. Chemically induced (e.g., ibotenic acid) lesions in MT create retinotopic defects that interfere with tracking eye movements, both smooth pursuit and catch-up saccades, to targets moving in any direction within the affected visual field; saccadic eye movements to stationary targets are unaffected.240 Lesions of MST, in addition to creating retinotopic defects such as those created by MT lesions, but with somewhat larger fields, can produce directional defects with lower smooth pursuit gain of targets moving toward the lesioned side no matter where within the visual field the target is located.241 Slow phase velocity of OKN toward the side of the MST lesion was reduced in both the initial (direct) component and the velocity-storage (indirect) component. Inferior Parietal Cortex DESCRIPTION. Two regions with documented oculomotor function: 7a, along the posterior inferior parietal lobule, and LIP neighboring 7a along the bank of the intraparietal sulcus (see Fig. 42). This area is also referred to as the posterior parietal cortex. INPUTS AND OUTPUTS. LIP and 7a have somewhat different connections. Thalamus (reciprocal): LIP primarily with pulvinar, but also with DM and VL; 7a primarily with pulvinar, LD, and LP, but also with DM, VL, and VA. Cortex (reciprocal): LIP with 7a, 7b, visual association cortices (V2, V3, V4, PO), occipital temporal association cortex (MT and FST), FEF, SEF, prefrontal and limbic areas; 7a with LIP, visual association cortex (V2 and PO), temporal association cortex (STP), FEF, prefrontal (e.g., area 46) and limbic areas. Striatum: Both LIP and 7a project strongly to caudate (head and body) and more sparsely to the putamen. Superior colliculus: projections from LIP, strongly; from 7a, less so. Pontine nuclei: projections from LIP and 7a. (See Cavada and colleagues242 for review.) MICROSTIMULATION. Electrical stimulation of the anteromedial part of area 7a elicits saccades with contraversive horizontal components usually of a particular size and direction depending on stimulus site.243 Whereas electrical stimulation of the FEF powerfully evokes saccades whether the animal is actively fixating or not, stimuli delivered to area 7a rarely evoked a saccade when the animal actively fixated a visual target. Frontal Eye Field DESCRIPTION. In monkey, the FEF is located anterior to the arcuate sulcus in area 8, but human studies place it in Brodmann area 6 near the junction of the superior frontal and precentral sulci. Saccadic and smooth pursuit subregions exist. INPUTS AND OUTPUTS. Five descending fiber bundles: to striatum, predominately head and body of caudate; to claustrum through external capsule; transthalamic and subthalamic fibers to thalamus (DM complex), subthalamus, and tegmentum of the midbrain (lateral mesencephalic RF) and pons (nucleus raphe interpositus and PPRF); pedunculopontine fibers to ipsilateral pontine gray and NRTP; ipsilateral superior colliculus, topographically161,234; and reciprocal connections with SEF, dorsolateral prefrontal cortex, premotor cortex, inferior parietal cortex (dense), cortex in caudal one third to one half of the superior temporal sulcus.244 MICROSTIMUATION. Saccades or smooth pursuit elicited, depending on site. At saccadic sites, elicited saccades are conjugate, indistinguishable from spontaneous saccades and have contraversive horizontal components.245,246 Prolonged stimulation at a particular site generates repetitive saccades, all of nearly the same amplitude and direction and simultaneous stimulation of two nearby cortical sites elicits a saccade intermediate between the saccade elicited by each site alone.245 Saccade amplitude is topologically ordered across the FEF, with large saccades elicited dorsolaterally and small saccades ventrolaterally.246 Elicited saccades corresponded to the natural saccade for which the cell, at that site, responded best.246 A separate zone, deep in the anterior banks of the arcuate sulcus, has been associated with smooth pursuit eye movements. Neurons in this region preferentially respond to smooth pursuit of a small, moving visual target and electrical stimulation of this region produces smooth pursuit eye movement that usually lasts for the duration of the stimulation.246,247 Initial acceleration and peak velocity of elicited pursuit increased with stimulation intensity, whereas movement direction depended on stimulation site.248 NEURAL RECORDINGS. Activity of isolated neurons related to eye movement have been recorded in the FEFs. Activity of most cells were strongly associated with goal-directed saccades, as opposed to spontaneous saccades, and most of those responding did so before the saccade began. These presaccadic neurons variably had a visual activity field, a movement activity field or both.249 Cells projecting to the superior colliculus preferentially had movement fields.250 LESIONS. Saccades and smooth pursuit are disturbed. A transient reduction in the frequency of saccadic eye movements toward visual targets in the contalateral visual field after unilateral FEF lesions recovers to near normal within 1 month.218 Horizontal and vertical smooth pursuit gain, too, is transiently reduced after FEF lesions.251 Dorsomedial Prefrontal Cortex DESCRIPTION. Because of its proximity to the supplementary motor area, this localized region of the superior frontal gyrus has been called the SEF (see Fig. 42). NEURAL RECORDINGS. Bursting neural activity in the dorsomedial frontal cortex precedes saccadic eye movements.252 MICROSTIMULATION. Saccades elicited in a preferred direction. OUTPUTS. Brain-stem projection of the SEF includes the superior colliculus.206 Dorsolateral Prefrontal Cortex DESCRIPTION. The primary location is Brodmann area 46 (see Fig. 42). INPUTS AND OUTPUTS. Reciprocal connections with FEF253 and the anterior bank of the superior temporal sulcus, middle portions project to DM thalamus254; and to the head and body of caudate, sparsely to putamen.255 NEURAL RECORDINGS. Many neurons latch target position in delayed memory guided saccade test.256 Most cells coded stimulus position irrespective of pro- or antisaccade task, whereas others coded response position.257 LESIONS. These usually produce deficits in memorization of visuospatial information in humans.258 SUMMARY OF VESTIBULAR AND OPTOKINETIC EYE MOVEMENT NEUROPHYSIOLOGY Eye movements arising from vestibular and optokinetic stimuli collaborate to steady gaze in space despite head movement. The vestibular system alone is insufficient to do the job because the peripheral vestibular signal dies away during stimulation (see Fig. 40). The OKS alone, too, is insufficient because of delays in processing the visual signals. Neural recordings have demonstrated that, at least for horizontal eye movement, both vestibular and optokinetic signals are processed in the vestibular nuclei (Fig. 43).
SUMMARY OF SACCADIC SYSTEM NEUROPHYSIOLOGY Neurophysiologic research has gone a long way in determining the neural events leading to a saccade; Figure 44 depicts the basic scheme. Neural structures have been associated either with target selection or with saccade execution. A saccade's execution involves creating the temporally encoded pulse-slide-step and pause-slide-step signal found in the ocular motor nuclei. The signal arises from a combination of separate pre-motor inputs. The pulse is generated by EBN located in the paramedian pontine RF for horizontal gaze (Fig. 45) and the rostral interstitial nucleus of the medial longitudinal fasciculus (riMLF) for vertical saccades (see Fig. 34). The pause is generated by IBNs located in the caudal pontine and rostral medullary RF for horizontal gaze and in the riMLF for vertical gaze. Interestingly, the preferred directions for these burst neurons align with the muscle-pulling/vestibular-canal directions.259 Activity of theseburst neurons is strongly related to the saccade's metrics: the saccade and burst duration for saccades larger than about 5 degrees is equal; peak burst frequency reflects peak saccadic velocity; and the total number of spikes in the burst is highly correlated to saccade size.260
Where the step part of pulse-slide-step signal originates is not known conclusively. Most likely, it derives from the vestibular and prepositus nuclei that contain neurons carrying an eye position signal (in addition to a persaccadic related signal) and project to the motor nuclei. Similar activity related to vertical gaze has been recorded in the NIC, which projects directly to the oculomotor nucleus.261 The source of the slide component is less well known but appears on those eye-movement related neurons in the medial vestibular nucleus.262 Another reticular cell, the omnipause neuron, discharges tonically at high rates except for pauses during saccades that, through direct inhibitory connections, squelches tonic activity in the burst neurons activity in the burst neurons (see Fig. 45). Exactly how OPNs are triggered is not yet known. In contrast to the temporal coding within structures involved with saccade execution, structures involved with target selection have a place code; the saccade direction and size are encoded by the cell's topographic location. Of these, the superior colliculus and FEFs can each trigger the brain-stem saccade generator. Pathways from the retina subserving visually guided saccades feed into the system by way of the lateral geniculate or superior colliculus. Lesions of the medial longitudinal fasciculus lead to an internuclear ophthalmoplegia affecting the contralateral medial rectus. PROPRIOCEPTION AND EFFERENCE COPY After the brain knows where the eye is pointing, then the extremely accurate calibration of the retina provides localization relative to the straight-ahead foveal direction. The problem for the visual system is, “How does the brain know where the eye is pointing?” Further, how does it keep track of when eye position changed and by how much it changed, and how does the brain properly assign movement of retinal images to either target movement in space or gaze changes? There are two general explanations of how eye position is registered internally. The first was proposed over 125 years ago by Helmholtz: The effort of will (out-flow or efference copy) to move gaze 5 degrees to the right, say, was also transferred to the visual system, alerting it to expect the visual field to change 5 degrees.3 Sherrington alternatively proposed that extraocular muscle tension or length information (inflow) might be signaled back to the visual system.263 The evidence is in favor of Helmholtz despite the existence of eye muscle proprioceptors. Muscle spindles, which could signal muscle length are abundant in humans, with 47 located in one inferior rectus.264 In addition to spindles, there are palisade endings265 along extraocular muscle tendons that could measure extraocular eye muscle tension. The cell bodies of these afferents are in the ipsilateral trigeminal ganglion266 and project to the ipsilateral sensory trigeminal and cuneate nuclei.267 How the brain uses these signals is not yet known. A myotatic stretch reflex, for example, does not exist in primate extraocular muscle.268 Efference copy is not provided by motoneuron collaterals269 but likely arises from widespread premotor distribution (see, for example, earlier discussions of vestibular and prepositus termination sites). Normally, visually guided eye movement uses a more accurate registration of efference copy than perceptual centers do, the latter relying more on visual input when available.270 For those with infantile nystagmus, however, efference copy is implicated as a mechanism used to achieve spatial constancy.271 PHARMACOLOGIC RESPONSES All neuromuscular junctions of extraocular muscle appear to be cholinergic in nature. Acetylcholine (ACh) is the normal chemical transmitter. With each nerve impulse, vesicles of ACh are released into the neuromuscular junction area and combine with the receptor protein on the muscle. In the twitch-type extraocular muscle fiber, this membrane depolarization propagates along the muscle membrane and down into the muscle through transverse invaginations of the muscle membrane, the T system. In most multi-innervated muscle fibers, the membrane depolarization remains localized, causing only local muscle contraction; it does not propagate all along the muscle fiber. AGENTS USED IN ANESTHESIA Blocking agents, curare and its analogues, combine with the receptor protein at the muscle site of the neuromuscular junction and thus compete with ACh. This involves all types of muscle fibers. This type of agent does not cause depolarization of the muscle, simply paralysis. Depolarizing agents, such as succinylcholine, both depolarize the muscle membrane and interfere with its repolarization. Like other muscle fibers in the body, the extraocular muscle twitch fibers give one or two twitch contractions on use of this drug but are thereafter inactive, because they cannot repolarize to allow further contraction. In multi-innervated fibers, however, local areas of depolarization mean local areas of muscle contraction; these are maintained by succinylcholine depolarization. This results in substantial increase in extraocular muscle tension, up to a third of the total muscle strength. This technic of activating the muscles under anesthesia has been employed to test muscles in strabismus.272 The effect of succinylcholine contracture increases the stiffness of the extraocular muscle.273 The effect lasts up to 30 minutes in humans in whom we have measured the length-tension characteristics of the muscle or electrically stimulated the muscle directly. This may confound determination of muscle stiffness at strabismus surgery, and should be avoided when assessment of abnormal muscle stiffness is important. Tranquilizer drugs can slow saccadic eye movements. Because this also occurs from lesions in the brain stem, it seems likely that the brain stem is the site of action of these drugs, most of which act by altering synaptic transmission. Anesthesia or sedation using these agents alters eye muscle tonus and eye alignment so that assessment of true surgical outcome may be unreliable for many hours after surgery. BOTULINUM TOXIN In strabismus, direct injection into overacting muscles of botulinum toxin (BT) blocks neuromuscular conduction for days to weeks and is used therapeutically.274 Botulinum toxin interferes with the ACh release from the nerve terminal.275 The BT molecule has three separate domains. The first binds selectively to receptors on cholinergic nerve terminals. With endocytosis, the BT ends up within vesicles in the nerve terminal. A second domain of the molecule expedites liberation of the BT into the nerve cytosol, where the third domain acts as an enzyme, selectively cutting one of several proteins responsible for exocytosis and the release of acetylcholine. Temporary paralysis of the target muscle changes alignment. If this alignment change is maintained for several weeks, the injected agonist lengthens and the antagonist contracts. In about 60% of cases, the effect persists after the initial paralysis resolves, which results in a long-term change of alignment. ACETYLCHOLINE Direct injection of Ach can be useful to stimulate contraction of eye muscles at surgery.276 This contraction may aid recession operations in which anesthesia prevents adequate tension from central innervation. CENTRALLY ACTING DRUGS Barbiturates interfere with smooth pursuit movement of the eyes. Because smooth movements can still be elicited by vestibular stimulation, this effect is presumably cortical in origin.277 Alcohol leaves saccadic and other brain-stem gaze functions intact, but it alters vergence tonus and creates a shift toward esophoria, with actual diplopia for fixation at distant targets in many subjects.278,279 It also increases central processing time and thereby interferes with accurate tracking and saccadic eye movements. Marijuana creates a similar tendency toward esophoria but substantially less alteration of gaze control function.280 Anticholinergic drugs, such as scopolamine, can markedly reduce and even abolish nystagmus amplitude in congenital nystagmus and in spasmus nutans. Unfortunately, this occurs at drug levels that cause substantial side effects. |
| TOPICS IN CLINICAL OCULAR MOTILITY | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
NYSTAGMUS Physiologic nystagmus is the oculomotor response generated to appropriate physical stimuli, such as vestibular or optokinetic. Discussion of physiologic nystagmus can be found in previous sections. Nystagmus having no appropriate physical stimulus is called pathologic nystagmus. Table 3 presents a listing of recognized pathologic nystagmus categories including causes, when known.
TABLE 3. Nystagmus Categories in Conscious Patients
PHYSIOLOGY OF STRABISMUS SURGICAL PROCEDURES Most strabismus surgery tightens or loosens muscles in the muscle plane or moves the insertion (or, rarely, origin) to a new position, creating a different muscle plane and, therefore, different muscle effects. It is reasonable to ask whether muscles adjust innervation to the task of the new position, which allows them to learn to do something different. This has been carefully examined in humans and in monkeys, and no evidence for innervation change is found; all effect is probably mechanical.281,282 Inasmuch as passive tissues are a major load in movement, scars or other tissue restricting movement should be sought and removed when possible. About half the cases of strabismus are concomitant, that is, simple misalignments, with the eyes maintaining about the same angle of strabismus regardless of gaze direction or distance of fixation. The remainder are noncomitant, with variation of strabismus angle depending on distance of fixation or gaze position. For these, cliniciansdevise ingenious operations that affect some gaze positions more than others. RECESSION Recession operations constitute lengthening or loosening procedures. If the insertion of, for example, a medial rectus muscle is detached and replaced 5 mm posterior to the original, the tension on this muscle is reduced. In effect, the static locus curve of the muscle has been displaced down the static length-tension curves (Fig. 46). Because of the nature of the length-tension curve, muscle force is normally most decreased in the direction of the field of action of the muscle, adduction; the next greatest effect is in abduction, where the restriction effect of the medial rectus is significant; the least effect is in the primary position, where tensions and stiffness are lowest. Clinicians are aware that in esotropia, recession of a restricting medial rectus muscle may have the greatest effect in the opposite (abduction) field of action, even more than into the field of action. Recession operations or other effective lengthening procedures are often called “weakening” operations. Although muscle tension for any eye position has been diminished, the muscle remains entirely intact. The concept of lengthening or loosening, rather than weakening, is a helpful view to maintain.
RESECTION Resection operations constitute shortening or tightening procedures. The static locus curve in Figure 46 is displaced upward along the length-tension lines. For an eye in esotropia, the lateral rectus muscle is usually thinner than the medial rectus muscle, which is stiffer and stronger. Thus it is no surprise that a 5 mm resection creates less angular change than a 5 mm recession. Large resections may exceed the tendon length and actually remove elastic muscle tissue, which increases muscle stiffness and reduces amplitude of eye movement. HOW MUCH TO DO Because muscle and tissue forces are found to be variable and cannot be measured in an individual case, simple formulas relating degrees of correction to millimeters of surgery are only general guides, and the result of surgery is predictable only within broad limits.283 The amount of surgery to do and still remain within the linear elastic limits of the muscles to allow 30 degrees of rotation each way is not over 7 mm for one muscle and 12 to 13 mm for a pair, such as the medial rectus and the lateral rectus muscles taken together. When these limits are exceeded, the amount of incomitance increases, inasmuch as one eye cannot match the excursion of its fellow. Surgery on more muscles, rather than more surgery on fewer muscles, helps preserve comitance—obviously while extending the financial cost of the surgery and prolonging its duration. Of course, limits much greater than 7 mm are often required in noncomitant strabismus, and limits much smaller than 7 mm are often dictated by the arc of contact, alteration of lid position, or other clinical considerations. Resolution of these competing goals constitutes the art of clinical surgery. THE EFFECT OF THE ANTAGONIST If, say, the lateral rectus becomes paralyzed and remains so, effectiveness of the recession of the medial rectus to correct the esotropia is reduced, given that the slack is not taken up. On the contrary, if the antagonist is extra stiff and strong (as is the case with endocrine exophthalmos), then the effect of recession is enhanced. Thus, the status of the antagonist is important, and a balancing of forces is the concept to have, not just weakening or strengthening.284 Figures 47, 48, and 49 show some calculated muscle forces in normal incomitant strabismus and in lateral rectus paralysis.285
THE ARC OF CONTACT Muscle insertions are sometimes recessed to a position posterior to the point of tangency. Then, progressive loss of effective lever arm with rotation occurs in the muscle plane. Beisner has shown that this is a small effect near the primary position with most of the surgical weakening effect due to length-tension changes (Fig. 50). Such an effect can be deliberately created by suturing the muscle to the globe without recession (the Faden operation of Cuppers, Fig. 51).286 This weakens rotation into the field of action, but not in the primary position (see Fig. 46).
TRANSPOSITION OPERATIONS If both the medial and the lateral rectus muscle insertions are moved to the area of the superior rectus insertion, they will also produce a supraduction effect, instead of purely horizontal rotation.287 This operation corrects from 12 to 15 degrees of vertical strabismus, shifting 5 to 6 g of horizontal force from each muscle to create supraduction, which is a small fraction of the 50 g force created by the agonist muscle during lateral gaze; therefore, this operation hardly decreases the amplitude of horizontal gaze movement. The two muscles are at normal length or close to it; thus, horizontal alignment is unchanged, and the reciprocal innervation for horizontal gaze works well. Of course, these muscle insertions can also be transposed inferiorly; tightening or loosening operations can be done at the same time to correct horizontal strabismus. When vertical rectus muscle insertions are transposed in a horizontal direction (the Hummelsheim operation and its many variations) a lesser angular correction is usually seen.288 This is a consequence of the vertical muscles being smaller in cross-sectional area. Further, the stiffness of the antagonist medial rectus is usually abnormally high in cases in which temporal transposition is done (lateral rectus palsy and Duane's syndrome). ELEVATION OF MUSCLE INSERTIONS Elevation or depression of horizontal muscle insertions changes the normal stabilizing effect of the insertions working around the center of rotation. For example, if the medial rectus muscle is recessed and transposed superiorly (Fig. 52), then during upward gaze this point is translated backwards into the orbit, thus slacking off the medial rectus and reducing its adduction effect. Similar procedures may be applied to the lateral rectus; applications in some strabismus types are as follows.
ELEVATION OF THE MEDIAL RECTUS AND DEPRESSION OF THE LATERAL RECTUS INSERTION A combined operation of this sort has no net effect on horizontal alignment in the primary position (unless these muscles are also tightened or loosened) and no net vertical effect, because one muscle is elevated as much as the other is depressed.289 However, with upward gaze, the medial rectus muscle diminishes its tension, and the eye thus tends to abduct; the lateral rectus in upward gaze is tightened, which thereby increases abduction (Fig. 53). With downward gaze, the medial rectus is tightened; the lateral rectus slackens. This would be effective in a case of strabismus in which the eye tended to be more esotropic in upward gaze or more exotropic in downward gaze (the A pattern). These muscle origins are far posterior, so that moving the insertions does not create much change in the angle they make with the visual axis. Thus, when these muscle insertions are changed, a minimal torsional effect results.
Depression of the medial rectus and elevation of the lateral rectus insertion is effective if esotropia tends to increase in downgaze and exotropia tends to increase in upgaze (the V pattern). BILATERAL ELEVATION OR DEPRESSION OF MUSCLE INSERTIONS If both lateral rectus muscle insertions were surgically moved upward, then these muscle insertions would move posteriorly, and the tension would slacken in upward gaze, reducing abduction; they would then be moved forward with downgaze, tightening them and increasing abduction. This would be good for correcting the V pattern. Downward surgical movement of both lateral rectus insertions improves the A pattern. Elevation of both medial rectus insertions decreases adduction upward and increases it downward. This would also improve an A pattern. OBLIQUE MUSCLE TRANSPOSITIONS It is possible to alter the insertion position of oblique muscle points to tighten or loosen them or to move them anteriorly or posteriorly in the orbit.290 The effect of several placements of the superior oblique muscle insertions is illustrated in Figure 54 and defined in Table 4. In general, the more anterior such transpositions may be, the less vertical will be the infraduction effect and the less abduction effect. Indeed, as one moves farther forward, this muscle becomes an adductor and an elevator! A similar analysis fits the inferior oblique. Thus, weakening the elevation and abduction effect of the inferior oblique muscle are better achieved by recessing it and moving it anteriorly. With the calculation possibilities of modern computers, a rational mechanical analysis of these and many other maneuvers previously involving laborious calculation is now possible.291 By careful accumulation of clinical data, helped by accurate modeling, clinical prediction of surgical results will undoubtedly be aided by such an approach.
TABLE 4. Points of Insertion of Oblique Muscle and Degree
of Effect
*Plus values, abduction, infraduction, intorsion; negative values, adduction, supraduction, extorsion. Effect is expressed as percentage of rotation force around the three axes.
|
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
|
There are adjustments at many levels of operation to compensate for inequalities of the two eyes and changes in muscle formation or eye position. These are particularly relevant to strabismus. ALIGNMENT To maintain orthophoria, the basic tonus (the level of activity achieved for each muscle in the primary position) must change throughout life as the visual axes tend to diverge (see section on position of rest earlier in this chapter). Re-establishment of alignment after retina or orbit operations and the recurrence of phoria positions after surgical attempts at correcting strabismus are everyday examples that confirm the tendency to stability of the established tonic position. The position of the visual axes in animals and humans deprived of normal binocular vision from birth is usually strabismic, and the position of eyes that become blind or amblyopic in adulthood is often strabismic. CONCOMITANCE The program for eye movements may, in infancy, adapt and compensate for motor differences between the two eyes or imbalances of muscles in the same orbit. For example, in eight monkeys, the size of muscles in pairs (both medial recti) was found to vary up to 20% in weight, although there was perfect comitance of eye movement (Scott, unpublished data). Fink has shown large variations in eye muscle origins, insertions, and mus-cle plane angle in different normal individuals.292 Thus, some adaptation of innervation must occur to establish comitance. In adults, however, it seems that the program of gaze innervations to individual muscles of the two eyes, once established, is not subject to much adaptation. Cogan has commented on the lack of correction for the incomitance with aberrant regeneration of the third nerve.293 Metz and Scott have shown that switching muscle insertions does not result in changes of muscle innervation to compensate the altered functional position.281 GAZE FUNCTION Gaze function is highly adaptable. Discussion of plasicity in the vestibular, saccadic, pursuit, and convergence systems can be found in previous sections. |
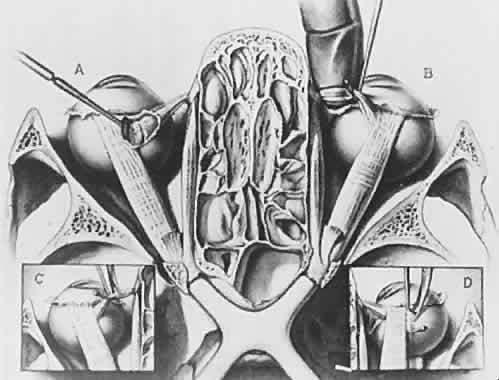
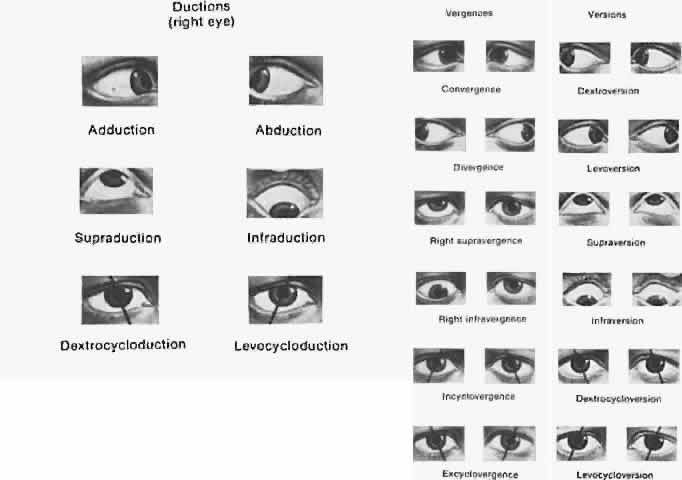

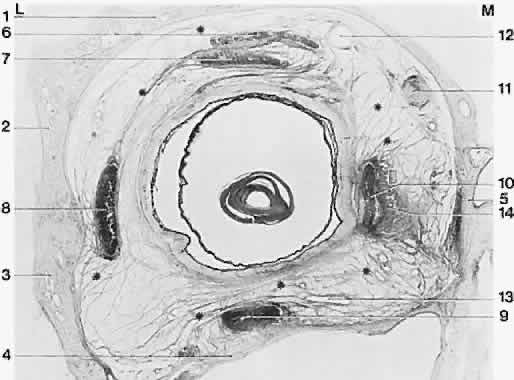


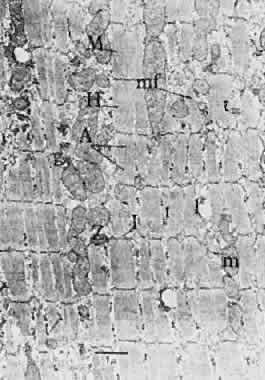
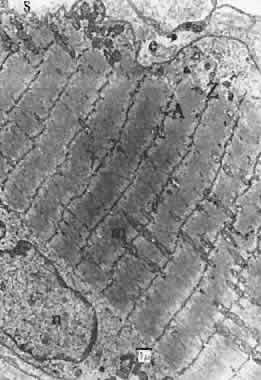
 2.718).
2.718).